
Bill White has a new monograph out: Post Traumatic Growth and Flourishing in Addiction Recovery: A Critical Review and Commentary.
Readers will know that I’ve long been concerned about the erosion of the boundaries of recovery.
My concerns center around a few issues.
Background
Recovery Management introduced recovery as a disruptor to the status quo of treatment providers organized around an acute-care model and marketing themselves with “recovery rates” based on 30-day follow-up calls, while failing to provide treatment and recovery support beyond stabilization. Recovery Management’s call for recovery-oriented care was intended to challenge the appropriation of recovery for professional interests and to raise the bar beyond short-term outcomes and beyond symptom reduction (remission).
Communities of recovery have conceptualized recovery as having a threshold for initiation (typically abstinence), typically confined it to severe cases of alcohol and other drug problems, and characterized it simultaneously as an ongoing process of change and as an endpoint.
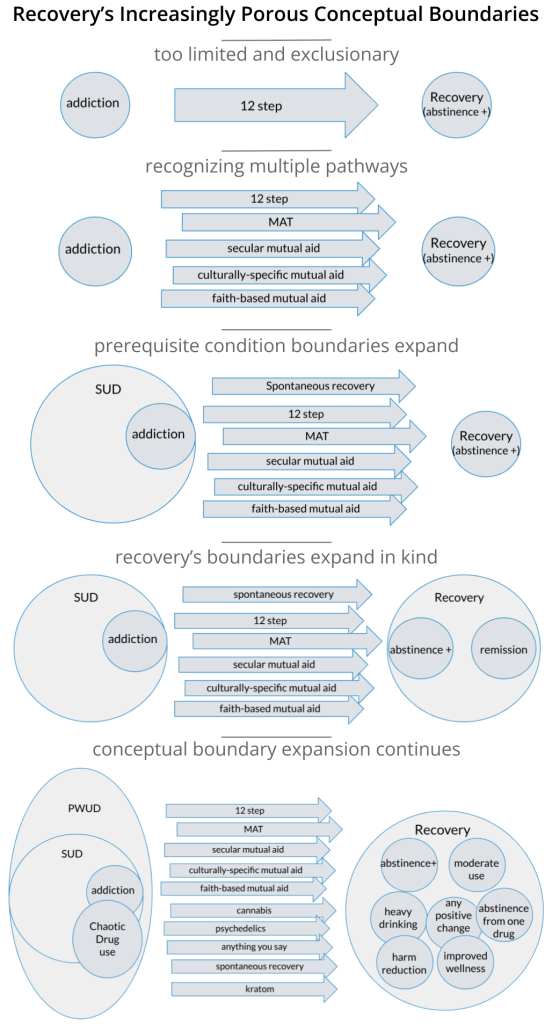
The adoption of a recovery paradigm has led to increasingly porous conceptual boundaries. Research, treatment, and public health professionals often reduce the threshold to any positive change.
Further, advocacy for the recognition of multiple pathways to recovery (a worthy cause) has manifested and evolved in ways that were not anticipated. We can think about pathways to recovery involving three elements: 1) a starting point; 2) a pathway; and 3) a destination.
All three elements have changed in ways that have made recovery more inclusive, but so broad and lacking in boundaries that recovery’s meaning has diminished to the point where it no longer raises the bar for patients and providers. In fact, it may lower the bar below remission. For example, if “any positive change” is recovery, then problematic drug use isn’t incompatible with recovery, and someone could make incremental positive changes and die of addiction while meeting a definition of recovery promoted by many researchers and professional helpers.
I’ve written many posts on the issue, but it’s clear the horse is out of the barn. Here’s why:
- We’ve seen a push toward a recovery paradigm at multiple interacting levels:
- treatment and recovery support (Recovery Management);
- system organization and change (Recovery-Oriented Systems of Care); and
- advocacy on behalf of people with addiction.
- Advocacy conferred status onto recovery and onto people associated with the recovery label.
- Recovery-Oriented Systems of Care elevated prioritization of recovery and the programs associated with the label.
- This association with cultural status/validation and social prioritization creates an untenable zero-sum dynamic with any effort to establish clearer inclusionary/exclusionary boundaries for recovery.
This leaves us in need of another paradigm to capture the “better than well” experience of recovery as it is lived in communities, and to raise the bar for professionals.
Flourishing is the strongest candidate to accomplish this.
The Flourishing Monograph
When introducing flourishing, White frames addiction recovery as a process involving:
- Subtraction – reduction of symptoms and impairment;
- Addition – improvements in global health and social functioning;
- Multiplication – “growth synergies that produce heightened levels of meaning and social contribution” producing a better-than-well recovery experience.
Multiplication is the part of the process associated with flourishing.
He contrasts flourishing with languishing, which is part of a spectrum he uses to describe the process of improvements (and deterioration) in global wellbeing and social functioning. Languishing may be one of the most important contributions to discussions of this issue. One can easily imagine many people on every pathway languishing while professionals pat themselves on the back and declare mission accomplished. Twelve-step members have long had a mental model for people who maintain abstinence but languish — the dry drunk.
The monograph’s Spectrum of Global Wellbeing and Social Functioning includes 5 stages that are described in more detail in the monograph.
- suffering
- languishing
- functioning
- growing
- flourishing
With recovery increasingly being framed exclusively as a process, flourishing provides an endpoint that is agnostic with respect to pathway and diagnosis. Sidestepping these issues is no small matter. With the boundaries of recovery becoming so diffuse and inclusive, I’ve repeatedly suggested that quality of life might be a better goal. (Concern about languishing motivated this sentiment, but I didn’t have that language.) Flourishing has the advantage of avoiding celebrating small, incremental QoL improvements as the endpoint, even as the person languishes. If flourishing is recognized as an achievable endpoint, we can see what approaches (or sequences of approaches) facilitate flourishing and which do not.
Importantly, flourishing isn’t framed as an individual endeavor—it is nested within family systems, community spaces, cultural contexts, and social determinants of health. This demands that providers look beyond the individual clinical level. In this framework, factors like family dynamics, community connection, and recovery-supportive cultural spaces are flourishing variables, not peripheral concerns.
Another important message is made clear in the discussion of recovery as an act of rebellion — that people in recovery must be active agents in their own recovery. This message is important beyond the context of recovery as an act of rebellion because flourishing is not something that can be delivered to passive recipients. In fact, agency is probably a defining quality of flourishing–flourishing demands wrestling with questions about one’s place in society and calls upon us to be of service.
It reminds me of a comment from a colleague 25 years ago when we were developing a program for adolescents with SUDs in the juvenile justice system. She said that we could view these kids as predators, victims, or resources. Further, society views them as victims and predators, and it was on us to meet them with the expectation that they can be resources within their families and communities.
Wrapping Up
White concludes with a powerful statement: recovery pessimism may be the primary barrier to flourishing.
Recovery pessimism is the lie that must be forever expunged from cultural consciousness. The reality, revealed by a growing body of scientific research and legions of people putting a public face and voice on recovery, is that: 1) sustained SUD remission is a widespread phenomenon—the normative outcome for substance use disorders, 2) SUD remission is often accompanied by enhancements in global health and social functioning, and 3) many people in SUD remission/recovery go on to experience lives of significant achievement, community contribution, and personal meaning and fulfillment, the true prevalence of which is limited by the lack of definitive studies of recovery flourishing. Recovery flourishing will increase when the dominant cultural narrative about the likely course of addiction, the prevalence of recovery, and the potential of recovering people as community assets are fully recognized at personal, public, and policy levels.
White, W. L. (2026). Post Traumatic Growth and Flourishing in Addiction Recovery: A Critical Review and Commentary. Chestnut Health Systems/Lighthouse Institute, Recovery Research Institute.
I’d argue that recovery pessimism is not something that lives outside of addiction and recovery spaces. There are plenty of people within research, public health, treatment, and advocacy who approach the work with pity for people with addiction and too much acceptance of languishing.
White’s monograph also has the potential to challenge those tendencies and revitalize Recovery Management, which has been overshadowed by and conflated with Recovery-Oriented Systems of Care.
It’s an important and much-needed contribution to the field. It also seems to be coming at the right time, as we may be increasingly ready to recognize the limitations of acute care models, medical models, public health, and harm reduction. It’s well worth your time.

Great post! I agree about the importance of raising the bar and believing deeply about the capacity of individuals to change and grow. “Nobody rises to low expectations” Goethe Mark Sanders
LikeLiked by 1 person