

This blog has had several posts on drug use, addiction, liberty, and involuntary treatment.
I’ve used the expression, borrowed from Keith Humphreys, of choosing between “hands on” and “hands off” approaches.
A recent article focuses on the use of involuntary Substance Use Disorder treatment under limited circumstances. This is toward the far end of hands-on approaches.
Rohan’s mother, he discovered, had applied to have him committed to a drug-treatment centre under a Massachusetts state law known as “Section 35 .”
Rohan spent the next 45 days at a treatment facility inside the county jail. There were relapses and four more committals in the years afterward. But he says that first stint planted a “seed of hope” that grew steadily. He’s been clean for two years, has started a family of his own and is holding down a rewarding job. Rohan, 36, unequivocally credits the state’s involuntary treatment program for rescuing him from a “suicidal” addiction.
“The program itself saved my life,” he says. “Without a doubt (if not for the program) I’m sure I would be dead … The day-to-day life of an addict is a million times crueller than getting handcuffed.”
Life of an addict “a million times crueller” than mandatory drug treatment. (2025, November 16). Unpublished.
The article includes arguments against this kind of aggressive hands-on approach. It references a paper on the experiences of Section 35 patients. That article includes this description of the most common criticism.
The involuntary aspect of ICC, compounded by the carceral facilities into which participants in Massachusetts were randomly placed, are trauma-inducing, not trauma-informed approaches. PWUD often have traumatic histories with the criminal justice system (McKim, 2017; Walt et al., 2022) and may avoid processes like ICC as a means of preventing further exposure to psychological trauma (Baigent, 2012; Santucci, 2012). Continued research is needed to further examine the ethical considerations of coercive treatment as well as its ability to effect longitudinal treatment outcomes and mortality risk reductions to PWUD who are involuntarily placed into treatment (Christopher et al., 2020b; Coffey et al., 2021; Evans et al., 2020; Mackain and Lecci, 2010).
Silcox, J., Rapisarda, S. S., Hughto, J. M. W., Vento, S., Case, P., Palacios, W. R., Zaragoza, S., Shrestha, S., Stopka, T. J., & Green, T. C. (2024). Views and experiences of involuntary civil commitment of people who use drugs in Massachusetts (Section 35). Drug and alcohol dependence, 263, 112391. https://doi.org/10.1016/j.drugalcdep.2024.112391
The risks and potential harms of an aggressive hands-on approach are real and should prompt serious discernment.
However, the risks of an aggressively hands-off approach are less frequently explicitly discussed. They are often assumed to be understood. The US’s strong norms around individual liberties often make hands-off approaches relatively invisible.
When arguments are made about harms associated with hands-off approaches, they tend to emphasize harms to communities. This article is unusual in that it presents a moral argument that isn’t rooted in the perspective of communities, grieving mothers, or even the public health imperative to prevent death. Instead this is a moral argument rooted in the suffering of people with addiction and the lack of parity with our responses to psychiatric crises.
Tanguay, head of Recovery Alberta, says his province has been working hard to tackle that shortcoming by increasing voluntary capacity. But he strongly defends the Compassionate Intervention initiative as a humane tool to help the most seriously ill users, people who lack the ability to seek out help themselves.
Tanguay notes that when a man threatened to throw himself off a Calgary bridge, the span was closed to traffic as firefighters, paramedics and mental-health professionals converged on the scene, eventually saving him.
“If that same person was under the bridge and injecting a lethal amount of fentanyl … we’d do nothing,” he says. “When it comes to addiction or substance disorders, we still have this inherent belief it’s a choice. It’s not a choice. For our most severe individuals, it’s imperative that we intervene.”
Life of an addict “a million times crueller” than mandatory drug treatment. (2025, November 16). Unpublished.
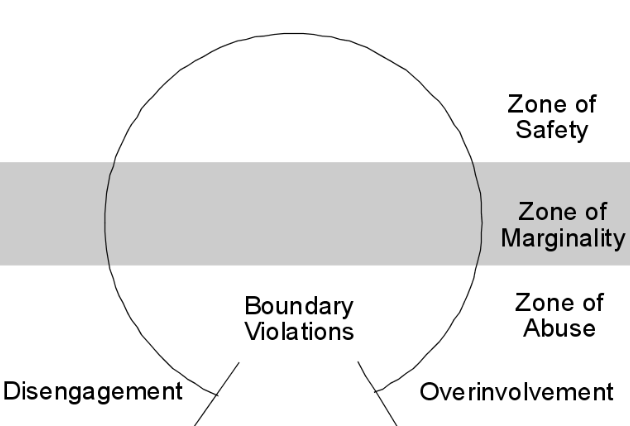
Bill White and Rene Popovits presented this image in their book Critical Incidents to illustrate the potential boundary issues tied to both overinvolvement and disengagement. It also captures the horseshoe effect of potential risks for hands-on and hands-off approaches. Professionals and policy-makers have a responsibility to recognize and mitigate those risks, whichever end of the spectrum their approach represents.
The example of Massachusetts’ Section 35 process (a very hands-on approach) points to some examples of failures to mitigate some of those risks. The article describes the use of jails for “secure treatment facilities.”
The psychiatric system isn’t perfect, but it’s a vast improvement over the use of jails for people who haven’t been charged with or convicted of a crime. It seems like Alberta may be taking that more seriously.
It’s hard to imagine the development of a system that includes limited secure, involuntary care while we maintain such cultural ambivalence about addiction as an illness and addictive drug use as a symptom of that life-threatening illness rather than an expression of free will.
I don’t know whether a decent, humane model is realistic. Psychiatric systems have blazed a trail that addiction care could follow. I spent several years as the director of behavioral health, so I had the opportunity to observe hundreds of involuntary patients and the process for their assessment, admission, legal hearings, treatment, and discharge. While involuntary admissions are often sad and difficult for everyone involved, and better systems of care in the community might have prevented the need for involuntary admissions, it seemed like the least bad option and I have no doubt it prevented death, disability, and serious crime, which may or may not set the patient on a trajectory toward flourishing, but it does interupt and hopefully prevent a trajectory headed toward disaster.
However, there is an important difference. Involuntary psychiatric admissions are relatively brief. In the setting I previously worked, most were less than a week. Alberta’s approach involves “three months in a residential treatment centre or six months in community-based treatment”, which presents much bigger challenges in terms of funding and development of programs, monitoring, and civil liberties.
