

Scotland, for all its beauty and positives, has an unwelcome first ranking in Europe in the domain of drug deaths. In 2021, the Scottish Government announced the National Mission as a response. A significant financial resource was realised to do this, spread over a variety of interventions. One of these was residential rehabilitation – a long-established treatment type, thought its provision appeared to be lower than in other European countries.
An investment of £100M (approx. $135M) over the five years of the planned National Mission was to be put into residential rehab to improve access, expand capacity and improve outcomes. The funding was a direct response to the recommendations of the Residential Rehabilitation Working Group. This expert group was set up by government to understand the provision of rehab, the pathways and barriers to it, its effectiveness and how we might better utilise it.
Those of us on the group supported the government to explore the field, assess the evidence, identify providers, understand pathways and to find out what barriers and conduits existed. The findings were of concern. We uncovered a postcode lottery of access, poor or non-existent pathways, a degree of professional and academic scepticism and a lack of outcome data. Most episodes of rehab appeared to be privately funded or funded through health insurance.
When we started, in much of Scotland, you had to be rich or lucky to get to rehab.
A lot of work has been done since then. Every Alcohol and Drug Partnership (commissioning body) in Scotland has developed a pathway to rehab, provision has been expanded, and a monitoring framework put in place to assess the impact of the investment in the sector. The evaluation of this part of the National Mission was the responsibility of Public Health Scotland (PHS), a part of the National Health Service.
Perhaps because we are a small country, or perhaps it’s simply on the grounds of willingness, it has been possible to get almost all of the providers of residential rehab (sitting across the private, third sector and NHS sectors) on board with data collection through a national dataset, rich with detail, to give a picture of what’s happening in rehab in Scotland.
PHS have been reporting at intervals on the number of publicly funded rehab places, but in the last week or so they have published their first ‘client-level’ data. These are early days, but there is cause for cautious celebration in the figures. What do they show?
Key findings
There were 870 publicly funded individuals in the sample analysed, covering the financial year 2023-24. Of that number, 42% started treatment for alcohol use and 32% for drug use. 26% were for both alcohol and drugs.
Where do residential rehab clients come from?
Just under half of individuals were referred from another substance misuse service. A quarter were referred from the NHS and 14% self-referred. Which parts of Scotland they come from is, frustratingly, not reported.
How long were they in treatment?
On average people waited six weeks or so to be admitted and treatment episodes lasted around two months – though where people didn’t leave earlier than planned, this rose to about three months. 95% of those treated in the period had only one admission
Who were they?
Two thirds of those accessing rehab were male. The median age was 43, slightly lower than the median across other treatments (47). If the problem was alcohol, you were likely to be older (49 for alcohol, 36 for drugs). The population was 86% white. Alarmingly, only 0.4% reported other ethnicity, but there were missing data for 14%. (Scotland has a 96% white population).
What were their circumstances?
Almost two thirds were unemployed and only half were in secure housing – something more likely if someone was starting treatment for drug use. A third had children under 16, but only 14% had a child living with them. Almost one in ten came to rehab from prison or had recently been in prison.
80% came from urban areas with just under half coming from the 20% most deprived parts of Scotland.
More than half had a diagnosed or suspected mental health condition. About one in three individuals starting a placement had had a previous overdose.
How were they funded?
92% of placements funded through a single public source of funding (ADP, local authority, housing benefit or health board) with the remaining 8% coming from mixed public funding sources
The median cost of a placement was just under £10,000 ($13,000), but for treatment complete categories (84 days duration) this was £13,334.
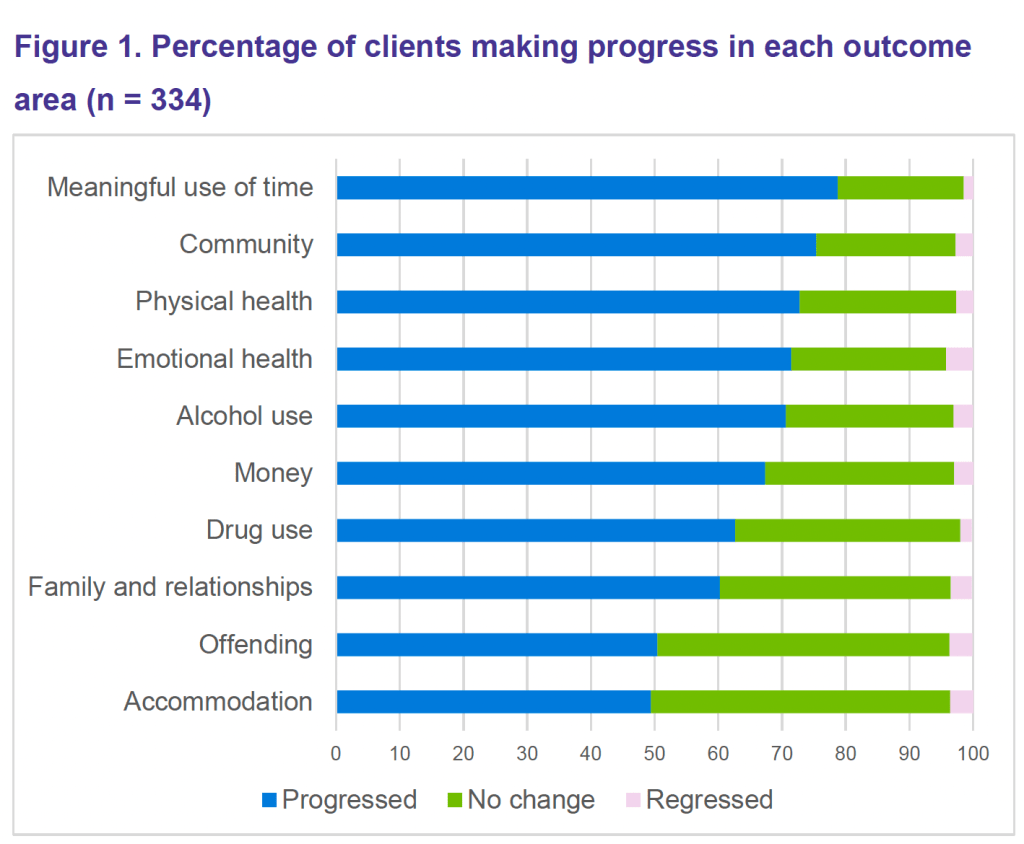
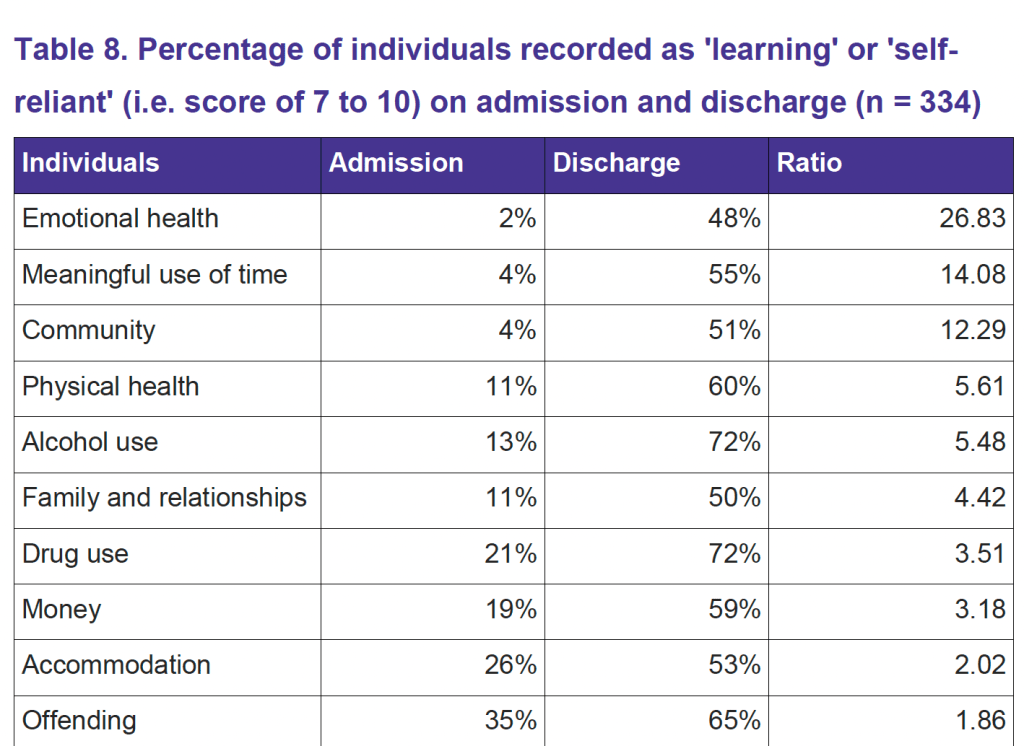
Did people get better?
Using validated tools, PHS analysed the data for evidence of progress in treatment across a range of outcomes. 85% of individuals made improvements in at least three domains of the Outcome Star. The areas with the most progress included meaningful use of time, community and physical and emotional health.
(Table from Public Health Scotland)
The ‘before and after’ data do look encouraging and are testament to the work of staff and clients in rehab settings.
(Table from Public Health Scotland)
Risk of death
One concern raised frequently about rehab, where the goal is abstinence, is the risk of loss of tolerance in opioid users, relapse and overdose. PHS analysts obtained a snapshot of risk of death in the drug using population in the sample – addressing the worry that rehab would be associated with an unacceptable risk of death. In this analysis one person died in the six months following discharge (0.7% of the sample). Non-fatal overdoses were not measured.
This is an early analysis and limited. Because all-cause mortality is high in this population over time we will need longer term data and also a comparison with community treatment and no treatment, but this goes some way to reassure individuals, families and the professionals working with them that there is unlikely to be immediate or high risk.
Who does best?
Those with alcohol problems; women; older age groups tended to do better.
Deprivation was not a predictor of completion, but there was a link with more secure housing status. Mental health problems did not strongly predict poorer completion. Employment was strongly linked to completion.
Waiting time to treatment did not affect completion rates. This is something that is often cited as a problem, but while waiting too long might generate other issues, it doesn’t look as if it causes poor completion.
Who doesn’t do well?
A headline finding was those who self-referred had the lowest completion rate, suggesting that the work done and support given to those referred by workers or professionals were important investments.
How did the Scottish Government do with its rehab programme?
Did the SG achieve its goal of 1000 publicly funded placement ahead of the 2026 target? Probably (in 2023-24) is the answer. There were 1037 placements cited. Though this figure included some clients from England, it may have missed some Scottish clients attending rehabs which were not reporting data.
Did access increase? Slightly is the answer, but the nuance is important – access to publicly funded placements skyrocketed – doubled in fact from 2019/20 to 2023/34.
Conclusions by PHS
- Individuals are making positive short term outcomes after rehab
- Drug-related deaths look to be low
- There’s been a 50% increase in Scottish residents accessing rehab
- Publicly funded places have doubled
- The SG has probably reached or exceeded its target
Post National Mission
The data just published is encouraging, but as recovery journeys take place over much longer periods of time, we will need data going forward and I hope the Scottish Government continues to contract PHS to gather and publish figures after the National Mission concludes in Spring 2026.
What else do we need to record? It is curious that an analysis of referral source by ADP area is missing from this report. That information is available. How can we know if the postcode lottery still exists if this is not reported? This should be reported going forward.
Levels and quality of pre-care and aftercare need to be quantified, and how those relates to completion and longer-term outcomes. We need to better understand what predicts completion and what actions can be taken to improve this. An evaluation of aftercare should also include how effectively rehabs connect their clients to mutual aid and recovery community resources.
Consideration should be given to replacing the Outcome Star with a recovery-capital tool. A better understanding of the recovery journey means that we need to get better at following people over time across different treatments and supports and developing close links to create an integrated recovery-focused system. We also need to incorporate detox information – what part does detox play in access, what are the outcomes from detox, what is the quality/safety of it, and are different substances associated with different outcomes?
We’ve come a long way in a short time in terms of rehab and that’s thanks to policy, ministerial leadership and message – “everyone who needs it should have access to rehab” – and hard work from government officials, the members of the various iterations of the Rehab Working Group, Public Health Scotland and Healthcare Improvement Scotland colleagues, Scottish Families affected by Alcohol and Drugs, the Scottish Recovery Consortium, the Scottish Drugs Forum, SHAAP and the numerous individuals with lived and living experience (and their families) who contributed to the process.
We are in a unique position in Scotland. With ongoing commitment to rehab as a legitimate part of the treatment landscape, national reporting of data, a growing recognition of recovery journeys and of the part that recovery communities play, a policy commitment to join things up and an ongoing focus on making things better, the future looks brighter, not just for rehab, but for recovery from substance use disorders generally.
Ref: PHS ‘Evaluation of the Scottish Government Residential Rehabilitation Programme

Thanks David – it does look like good progress since the start of the national mission. As you say, the Outcome Star gives some positive indications of the impact of treatment, but is Scotland doing any research to measure verified impact on reoffending, employment, housing status?
LikeLike
Hi Mike. The DAISy dataset that Public Health Scotland uses to report on treatment captures some detail on prisons, employment and housing. There may be further research going on that looks at this in more detail, but I’m not aware of that. We published outcome data from the service I used to work in which covered some of those areas too.
LikeLike
Do you have any sober living environments for post treatment? If so, what is the required length of stay and what is the follow-up care in combination with housing? If so, do you have live-in supervisors?
LikeLike
Yes, there is a variety of recovery housing provision in Scotland, often linked to rehab providers. The Scottish Government undertook a mapping exercise of this a couple of years ago which you can find here.
LikeLike
Not to quibble too much, but just so we’re clear; Alcohol is a drug. No need to …..bifurcate.
LikeLike
Absolutely right – alcohol is a drug. Depending on what lens you look at it through (e.g., policy, treatment, regulation, effects, culture etc.) it can have different characteristics. Sometimes those lenses are helpful I guess and other times…
LikeLiked by 1 person
I have a fantasy that keeping the language simple–in this one area at least–no more alcohol and drugs or other drugs but just drugs, could open the culture up to understandings of our unconscious cultural ….dictates/rules/short-comings. But, I do feel–It’s All Good.
LikeLike
PS: I also have plenty of Scottish blood from my Mother’s side and feel deep love for my ancestral homelands—esp. when I watch that romantic yet effective Braveheart tale.
: )
LikeLike