
This guest post is by Lee Holley, LCSW, LCDC, PSS. Lee is a psychotherapist based in Texas. He specializes in therapy for people with alcohol and other drug problems through a recovery-oriented harm reduction lens, combining clinical expertise with lived experience in long-term recovery.
As a psychotherapist who bases my philosophy of treating alcohol and other drug problems on Jason Schwartz’s concept of “Recovery-Oriented Harm Reduction”, I expend a great amount of mental and emotional energy trying to practice both/and thinking instead of either/or in regard to the recovery and harm reduction worlds. This is further complicated by the fact that I am a person in long-term recovery, so I need to maintain my own anchors to recovery as I stay open to the fact that what worked for me might well be the exact opposite of what someone else needs. It’s a balancing act that feels especially difficult when the illicit and licit drug supply landscapes shift rapidly and drug policy becomes a front in the broader culture war.
With these facts in mind, the more recent introduction of 7-Hydroxymitragynine (7-OH) into the licit drug market – in Texas specifically, though it’s clearly happening nationwide – is of particular importance to me.
7-OH is an alkaloid derived from the plant Mitragyna speciosa, better known as kratom. In natural kratom leaves, 7-OH is present only in trace amounts, typically from 0.6% to 0.7%. What makes 7-OH especially notable is that it’s far more potent than mitragynine, the primary active alkaloid in kratom. Available pharmacological research estimates that 7-OH is approximately 10–20 times more potent than mitragynine at the mu-opioid receptor. In that way, it could be said that 7-OH is to kratom what THC-P is to cannabis – a minor natural constituent, but capable of producing disproportionately strong effects when isolated or synthesized.
All of this speaks to a discrepancy I’ve observed – while tobacco companies and some pharmaceutical companies are (rightly) vilified for knowingly pushing harmful, addictive substances onto the public, other suppliers – from underground chemists to gas station vendors – are sometimes positioned as life-saving harm reductionists simply responding to market demand. But in contrast to what the Drug Policy Alliance’s report on the role of drug dealers in harm reduction suggests, this framing often ignores the complicated, sometimes contradictory ways these lower level suppliers operate. At any given time, a drug merchant company or individual may be supplying drugs to people who…
- Are addicted
- Are using them recreationally
- Have a drug problem (not addiction)
- Are treating a mental or physical health condition
- Are trying them for the first time and will develop an addiction
- Any combination of the above
With all of these factors, drug merchants may be reducing pre-existing harm and / or generating new harm.
While kratom itself has a long history of use in Southeast Asia, where it’s been chewed or brewed into teas for stimulant and analgesic effects, these new, ultra-concentrated 7-OH products do not. I’ve seen reports suggesting a “seemingly improved safety profile of mitragynine compared to classical opioid agonists,” which sounds encouraging for pain management, but this is far from evidence that these other, novel, derivative products are safe. In fact, the arrival of semi-synthetic 7-Hydroxymitragynine products on the market represents the latest example of a pattern we saw in Texas with THC products: minor plant alkaloids being concentrated, synthesized, and sold with little research and even less oversight. And since kratom is legal in Texas as of September 2025, this pattern appears to be taking place independent of the substances’ legal status, raising questions about “The Iron Law of Prohibition.”
I’ve known several people who have struggled with 7-Hydroxymitragynine (7-OH), and while it may be safer than using illicitly manufactured pills, it still poses significant risks. Despite being marketed as a less harmful option, its potent effects have led these individuals to experience disruptions to their mental and physical health, withdrawal symptoms, and addiction. These outcomes demonstrate that what is a substance that reduces harm for one person is a dangerous entry point into addiction for another (similar to how vaping was introduced as a smoking cessation product but then marketed to teens and now has become stronger than ever.)
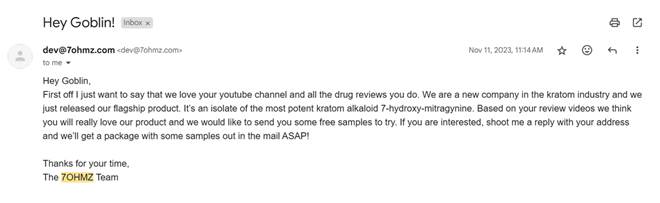
On 3/1/2025, @TheGoblinnn (a YouTuber known for drug storytime videos and a part of the drug commentary video niche) posted the following on X –
One of the owners of 7OHMZ, a leading 7OH brand, reached out to me and sent a text his Lawyer would probably kill him for.
He incriminates himself and the entire industry, suggesting there’s things he can’t “legally” tell me about their products and others. But he still wants to tell me about them; just not on a recorded line.
He then describes HIS OWN PRODUCT as a “Monster” that he helped create. He continues to tell me how he tried reaching out to me in the early days, and I found the email which I will attach below ⬇️
(See the X post here, or scroll below, to see the text exchange and email.)
This kind of backchannel admission – with the person describing 7-OH as a “monster” while previously having offered free samples and saying that Goblin would “really love it” – should be deeply concerning to clinicians, policymakers, and people who use drugs alike. It raises essential questions about where the line between harm reduction and harm production lies.
Texas has become something of a testing ground for this dynamic, with 7-OH extracts openly for sale in headshops, smoke shops, and gas stations. While some would argue this is part of a beneficial harm reduction strategy, which it very well may be, I would warn that we may be overlooking the long-term social and health consequences of leaving new, potent drugs largely unregulated.
While I’m open to the idea that language like “hard” and “soft” drugs can be overly simplistic or stigmatizing, it’s clear that not all drugs carry equal risk profiles or health impacts. Just as flavored liquor is qualitatively different from light beer in both strength and potential consequences, the same is true for substances like kratom compared to isolated 7-OH-mitragynine. This isn’t to say light beer or kratom are harmless or people can’t become addicted to them, but the risks associated with liquor and 7-OH are generally greater.
I think it’s important to have honest conversations about how some of these new “legal” products are being marketed, especially in spaces where people might be seeking relief from anxiety, pain, or cravings. Take a look at Hydroxie and Dozo Perks. Hydroxie sells flavored, chewable 7-OH products with smiley faces on the packaging and branding that reminds me of “roxies” – a term historically associated with oxycodone. Dozo’s “Perks” also lean into this pharmaceutical slang, more clearly referring to Percocets, packaged as with four servings per tablet, which really doesn’t make sense. One label even promises “instant relief” – relief from what, exactly? The marketing feels disingenuous, borrowing from opioid drug culture aesthetics while downplaying risks. It’s a good reminder that just because something is legal or branded with bright, wellness-friendly colors doesn’t mean it’s risk-free or ethically promoted.
The “all drugs are equal” framing flattens important distinctions around potency, dependence potential, routes of administration, overdose risk, and social impact. It’s possible to reject moralistic, binary labels while still respecting the complexity and gradations of harm that exist between different substances. Pretending otherwise isn’t compassionate – it’s dishonest, and it undermines public health messaging, recovery frameworks, and harm reduction efforts.
Jason Schwartz has written, “it’s not enough to ask whether a given intervention reduces harm in the short term — we have to consider what it does to the long-term ecology of our communities.”


What I appreciate here is the honest tension between harm reduction and harm production. But we’ve got to start from a different premise: people don’t have drug problems, they have drug solutions. A pill, powder, or plant is often meeting a need that was unmet elsewhere: pain relief, emotional regulation, connection, or escape.
That doesn’t mean those solutions can’t become problems. They can. But it also means outcomes vary across the spectrum, some people experiment with heroin or 7-OH and never develop an ongoing relationship with it, while others find themselves entangled. The difference isn’t just about chemistry; it’s about context, meaning, and the ecosystem of their lives.
Which is why I worry about flattening all drugs, or all suppliers, into the same frame. Just as not all substances carry equal risk, not all relationships to substances do either. When we treat every drug the same, or every use the same, we create belief systems that cause more harm than they prevent.
Public health messaging and recovery frameworks get stronger when we acknowledge this complexity. Compassion isn’t pretending everything is harmless, it’s telling the truth without reducing people to caricatures.
LikeLike