
As harm reduction has risen in prominence and influence in the addiction, treatment, and recovery spaces, one of its contributions to discussions about public policy related to drug use has been the suggestion that prohibition creates a drug supply with unpredictable potency that is vulnerable to contamination, and that these factors drive overdose. This leads to the conclusion that safe supply is a solution for the problem of overdose.
There’s no question that there is truth to this argument, AND it’s never been satisfying to me. Here’s why:
- It would certainly have the potential to prevent OD in the context of rational drug use, but a lot of drug use in addiction isn’t rational.
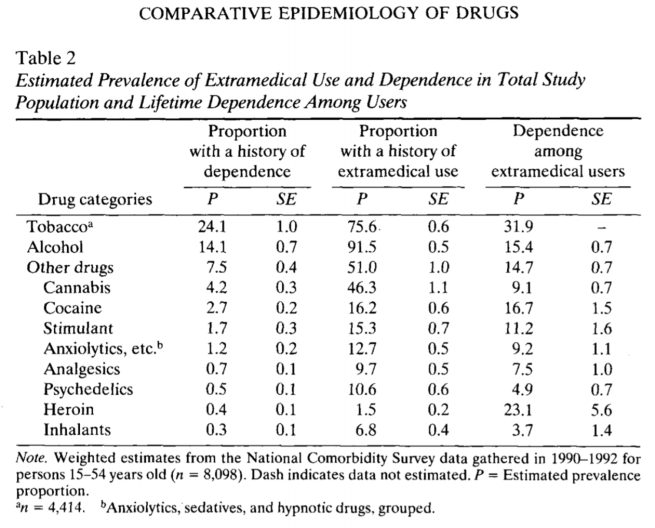
- Most drug users will not become addicted or develop a serious problem with a drug, but capture rates should be an important consideration that provide cause for concern about the possibility of policy change increasing the number of people using a substance.
- Capture rate = the % of users who will become chronic users of the substance.
- Regulation can contribute to a predictable supply, but it’s also true that our current legal and regulated drugs (alcohol and tobacco) are public health disasters.
- Regulated supply might make today’s substance of concern less likely to result in an OD, but drug use patterns aren’t static.
- Illicit drug supplies do change, sometimes suddenly, in ways that increase dangers, but a lot of what gets labeled as contamination is actually innovation to enhance the effects or reduce cost. Would this innovation stop in the context of a regulated supply? Wouldn’t stopping it require prohibition?
What’s your point?
Kratom has been a growing concern for some time. Kratom advocates say it provides effective pain management for many users and a pathway off opioids for others. I accept that this is true for some users, but I don’t know the prevalence. I’ve also seen kratom function as part of people’s addiction (often offering false hope for control of their addiction) and as a pathway to relapse for people in stable recovery from addiction. I also don’t know the prevalence of these patterns of use.
At any rate, kratom is legal in all but 6 states and Washington, DC (with Louisiana’s ban taking effect on August 1, 2025). Despite kratom being legally available in most of the country, we’re seeing innovation with the emergence of semi-synthetic products that are consumed through multiple routes of administration and contain up to 98% 7-hydroxymitragynine (7-OH) rather than the 1-2% of the previous generation of kratom products.
A letter published in the journal Addiction said the following:
The policy implications of semi-synthetic 7-hydroxymitraynine products are unknown, but adverse events or fatalities resulting from 7-hydroxymitragynine products could pose complications to the regulation of a growing kratom industry. Kratom is now used by 10–15 million US adults.
Smith, K.E., Boyer, E.W., Grundmann, O., McCurdy, C.R. and Sharma, A. (2025), The rise of novel, semi-synthetic 7-hydroxymitragynine products. Addiction, 120: 387-388. https://doi.org/10.1111/add.16728
Recently, 3 deaths in Los Angeles were attributed to 7-OH.
There’s a long history of hysteria in drug policy and drug coverage that has harmed citizens and failed to effectively protect communities. My intent is not to stir alarm. Rather, my point is that kratom is legally available and we’re still witnessing innovation to increase potency in a way that may increase the dangers and change the relationship between users and the substance.
This should raise suspicion toward arguments that regulated supply would stop dangerous innovations in the drug supply and use patterns. That isn’t the only argument for “safe supply”, but this example suggests that there may be no way to avoid prohibition, which invites questions about what we should prohibit and how we should do it, rather than whether to prohibit or not.
As I’ve written many times in this blog, these drug policy questions are all about trade-offs and acknowledging that every policy requires living with some problems. If that’s true, the questions you have to wrestle with are:
- Which problems are intolerable and which are you willing to tolerate?
- How do you make these decisions? (I’d suggest that even responses that purport to be value-free are value-laden.)
- Which policy (or combination of policies) best balances these values?
Below is a related post from last year.
Drug “poisoning” or “overdose”?

The NY Times has an article on the debate between characterizing drug deaths, fentanyl deaths in particular, as poisonings or overdoses. Much of the argument focuses on destigmatizing drug-related deaths.
“If I tell someone that my child overdosed, they assume he was a junkie strung out on drugs,” said Stefanie Turner, a co-founder of Texas Against Fentanyl, a nonprofit organization that successfully lobbied Gov. Greg Abbott to authorize statewide awareness campaigns about so-called fentanyl poisoning.
“If I tell you my child was poisoned by fentanyl, you’re like, ‘What happened?’” she continued. “It keeps the door open. But ‘overdose’ is a closed door.”
“Overdose or Poisoning? A New Debate over What to Call a Drug Death.” The New York Times, 2024, www.nytimes.com/2024/03/11/health/overdose-poison-fentanyl.html. Accessed 12 Mar. 2024.
One argument in the article is that this change in language creates “innocent” victims that will need to be contrasted with villains or guilty victims.
I’d also add that how we frame the problem determines how we frame the solution.
- Framing the problem as “poisoning” sets up “safe supply” as the solution.
- Framing the problem as addiction sets up treatment and recovery as the solutions.
- Framing the problem as a medical condition sets up a doctor as the solution.
- Framing the problem as a bio-psycho-social-spiritual condition sets up whole-person recovery and multidisciplinary medical and nonmedical interventions as the solutions.
- Framing the problem as crime sets up law enforcement as the solution.
- Framing the problem as public health sets up surveillance, education, and policy change as solutions.
- Framing the problem as stigmatizing language sets up language change as the solution.
- Framing the problem as criminalizing a health problem (driving people into the shadows) sets up legalization as the solution.
- Framing the problem as despair sets up social engineering or economic aid as the solution.
More than one thing can be true at the same time. There’s truth in both poisoning and overdose. It’s true that the drug supply has more unpredictable high-potency doses than ever before. It’s also true that this is nothing like the Tylenol poisonings and that, in some ways, fentanyl and tranq are innovations that serve a particular function rather than contamination — to ensure higher potency, lower price, and extend the duration of the effects of the drug.
We demonstrated that preference for fentanyl was increasing between 2017 and 2018 among our cohorts of PWUD who used opioids. In a multivariable analysis, younger age and daily crystal methamphetamine injection remained independently associated with preference for fentanyl. Most commonly reported reasons for preferring fentanyl included more euphoria, longer effects, and development of high opioid tolerance.
Ickowicz, S., Kerr, T., Grant, C., Milloy, M. J., Wood, E., & Hayashi, K. (2022). Increasing preference for fentanyl among a cohort of people who use opioids in Vancouver, Canada, 2017-2018. Substance abuse, 43(1), 458–464. https://doi.org/10.1080/08897077.2021.1946892
I believe that alcohol and other drug problems are complex with multiple dimensions and require comprehensive solutions that simultaneously address multiple dimensions. There may have been times when public discourse overemphasized addiction at the expense of other dimensions. However, I fear that many of the trending frames obscure the role of addiction and, in some cases, erase addiction. I tend to think “poisoning”, while it contains some truth, contributes to that trend. After all, the opioid crisis began with prescription opioids — a safe and regulated supply. And, alcohol and tobacco have massive social and health costs — safe, accessible, and regulated supply.

An example of this exact dynamic related to a legal and regulated drug is that of synthetic nicotine and the particular problems it brings.
https://recoveryreview.blog/2025/07/01/6-methyl-nicotine-is-here/
LikeLike
We keep looking to fix the supply without fully facing the why.
Yes, unpredictable potency and contamination increase overdose risk. But people don’t experience addiction because they stumbled into a toxic batch. They turn to substances because something in their system—emotional, relational, or spiritual—is asking for relief.
“Safe supply” might reduce immediate harm. But the deeper harm often starts long before the first pill, powder, or drink. It starts in disconnection. In trauma that never got processed. In nervous systems that never learned how to safely feel.
Kratom is a perfect example: legal in most states, yet already being modified to increase potency—and danger. That’s not contamination. That’s innovation driven by demand. And if we don’t address the demand, the chemistry will keep evolving.
We don’t need cleaner supply alone. We need to face the full complexity: pain, disconnection, craving, coping, and what it actually takes to heal.
Let’s not erase addiction in the name of policy. Let’s understand it so we can respond with something deeper than control.
LikeLike