

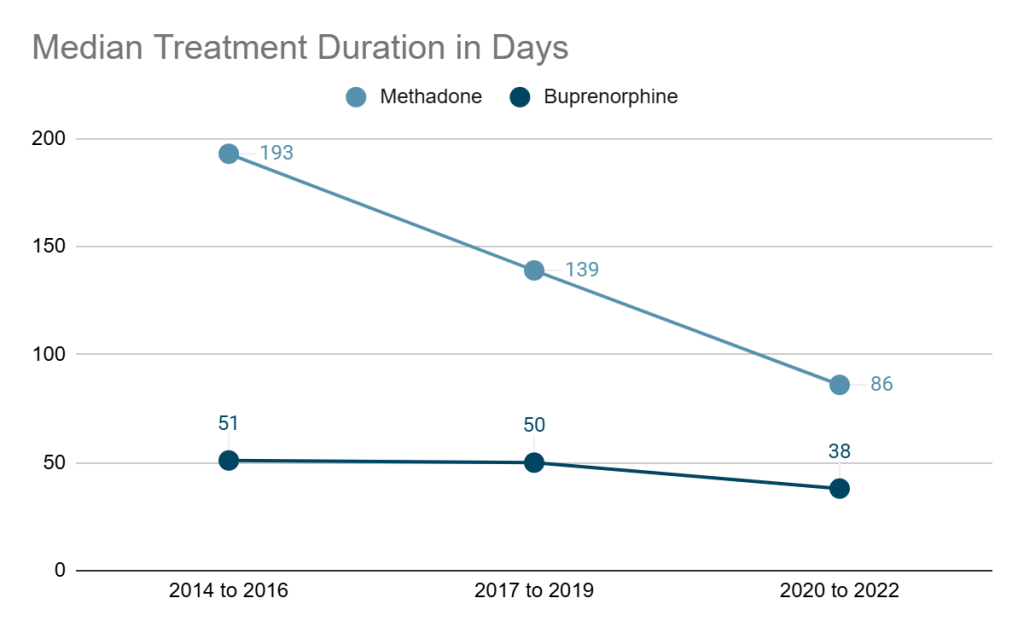
An eye-popping article was just published in JAMA about trends in the duration of methadone and buprenorphine treatment in Ontario, Canada, including more than 72,000 new recipients of opioid agonist treatments.
The median duration of buprenorphine treatment declined by 25%, from 51 days to 38 days.
The median duration of methadone treatment declined by 55%, from 193 days to 86 days.
25 years ago, Bill White challenged the field to abandon acute care models and replace them with Recovery Management and Recovery-Oriented Systems of Care. Like treatments for addiction to alcohol and other drugs, acute care models were the norm for people with opioid addiction.
Bill described the acute care model as follows:
Opioid addiction has been defined as a chronic, progressive illness for more than a century, but the treatment of this disorder, like the treatment of other addictions, has been conducted primarily within an acute care (AC) model of service delivery. The AC model is marked by five distinguishing characteristics. First, care is provided within self-encapsulated, crisis-oriented episodes of care, each of which is marked by screening, admission, intake assessment, a short series of treatment procedures, discharge (with, at best, short-term follow-up), and termination of the service relationship. Second, a professional expert directs and dominates the service delivery decision-making process. Third, services transpire over a short (and historically ever-shorter) period of time. Fourth, the individual/family/community is given the impression at discharge (“graduation”) that long-term addiction recovery is now self-sustainable without further professional assistance. Fifth, posttreatment relapse and re-admissions are viewed as the failure (non-compliance) of the patient rather than a failure of service design or execution.
However, opioid agonist maintenance treatments were believed to at least have the advantage of maintenance — the assumption that these treatments are long-term and will continue for years, possibly never to be terminated.
Where buprenorphine is concerned, that advantage never really materialized, at least not with consistent findings across studies. Retention is important in any treatment, but it became particularly salient during the opioid overdose crisis, when one of the strongest arguments for these treatments has been their effectiveness at protecting patients from overdose. In fact, this has been central in efforts to frame agonist treatments as the gold standard and discredit other treatments.
Recovery Management was initially disseminated around 2000 and sought to organize “addiction treatment and recovery support services to enhance early prerecovery engagement, recovery initiation, long-term recovery maintenance, and the quality of personal/family life in long-term recovery is described. The shift to a model of sustained recovery management includes changes in treatment practices related to the timing of service initiation, service access and engagement, assessment and service planning, service menu, service relationship, locus of service delivery, assertive linkage to indigenous recovery support resources, and the duration of posttreatment monitoring and support.” (White, 2008)
At that time, the field was consumed with competition between 12-step Facilitation, CBT, and Motivational Enhancement Therapy for recognition as the most effective treatment model.
Bill would admonish audiences that these arguments were taking place within the acute care paradigm, and that the acute care paradigm needed to be abandoned for the chronic illness of addiction. All therapeutic models delivered within the acute care paradigm will fail when applied to addiction.
Similar dynamics have emerged specific to treatments for opioid use disorder:
The professional treatment of OUD utilizes two broad approaches with varying levels of integration: 1) psychopharmacological treatment, and 2) psychosocial treatment. These competing but potentially complementary approaches are often nested within isolated silos of care with proponents of each claiming moral, clinical, and scientific superiority.
That competition manifests in arguments about gold standards, telehealth vs. “rehab”, residential vs. [fill-in-the-blank], agonists vs. antagonists, MAT vs. abstinence, harm reduction vs. abstinence.
In this context, it’s not at all shocking that overdose rates have remained stubbornly high despite massive investment in access to agonist medications and naloxone.
The most striking thing about substance abuse treatment is the mismatch between the duration of treatment and the duration of the illness.
DuPont R. (March, 2018) Interview with Brian Coon. Interview presented at the NC Recovery Alliance Summit, Durham, NC.
Consider the ongoing crisis, these disappointing retention rates, and outcomes measured in weeks and months that often focus on preventing adverse events rather than quality of life. A good example is a recently published Yale study on mortality and treatment type, where long-term treatment was defined as >21 days.
If Recovery Management and Recovery-Oriented Systems of Care were the reality, we wouldn’t be talking about agonist medications (or any other modality) as “treatment” — as though one modality or one episode is sufficient. Instead, we’d be talking about these treatments and interventions as entry points, stabilization tools, and/or recovery supports as part of a path from precovery to stable recovery to recovery maintenance. Instead, the field is consumed with arguments within frameworks that conflate entry points and endpoints.

I hope there is something left in treating substance use disorders with the magnitude of cuts about to occur from the loss of Medicaid funding. I love this field with every ounce of my being. People deserve to be treated with dignity and respect and get the care they need to recover from this disease. We are taking several steps backwards with this health administration and I am deeply concerned and afraid.
LikeLike
Great Post! Challenging us to address addiction as a chronic and progressive illness. Mark Mark Sanders
LikeLike
Here, hear, Jason . . .
LikeLike