
Notes:
This post features an AI-aided summary that condenses my 70-page master’s thesis, written in 2016, into a manageable 7,000-word essay. I never published the thesis, though I handed out copies to coworkers and friends. This was because, like many of my ideas, it grew voluminous rather quickly, and cutting it down to a manageable size seemed an impossible task to do by hand. The advent of LLMs has allowed me to forgo the struggle of condensing the work without losing too much. This LLM summary, however, does still reflect the limitations of such AI-aided summaries. So be nice, the robot worked really hard to make it.
While the model is, of course, limited by my understanding at the time, the intent was quite noble – to develop a synthetic theory that could bridge the gap between addiction and recovery concepts in a way that could explain the chief mechanisms of both. I relied heavily on existential psychology, terror management theory, and the role of self-esteem in the development of the work. I’m pleased that it still holds some relevance and has aged somewhat well. Hopefully, someone who reads it will find it either theoretically or clinically useful.
I also want to recognize Maia Fohman and Amada Bressack, with whom I spent many hours working, discussing, and writing about the original concept after graduation. Although the post-graduation project to publish this work never became what we had hoped, their input and labor were indispensable in the final iteration we did manage to achieve.
Critical Existential Theory of Addiction and Recovery (CETAR)
Abstract
This paper introduces the Critical Existential Theory of Addiction and Recovery (CETAR), a multidisciplinary framework that reconceptualizes addiction as a consequence of Critical Existential Failure (CEF)—a core disruption in the individual’s ability to derive meaning, sustain self-esteem, and mitigate mortality salience through symbolic and social processes. CETAR challenges the dominant biomedical and behaviorist paradigms that define addiction primarily in terms of substance use, proposing instead that addiction arises from existential dislocation, often rooted in developmental trauma, cultural marginalization, or a breakdown in symbolic coherence.
Drawing from existential psychology, Terror Management Theory (TMT), and clinical literature on spirituality and recovery, CETAR positions addiction as a maladaptive strategy to regulate mortality anxiety and restore symbolic meaning. In this model, substances are not merely chemical reinforcers but existential tools used to compensate for a failed capacity to generate meaning, belonging, and value. Recovery, accordingly, is not reducible to abstinence but involves an existential transformation through principled action, restored connection, and the reconstruction of identity within a socially embedded, symbolically coherent framework.
This paper outlines CETAR’s theoretical foundations, maps the trajectory of addiction and recovery through the lens of existential failure and mortality salience, and proposes new directions for empirical research and clinical practice. Specifically, it calls for the development of quality-of-life metrics and existential diagnostic tools that move beyond the use/non-use paradigm, offering a more comprehensive and human-centered understanding of both addiction and recovery.
1. Introduction
Despite decades of scientific advancement in addiction research, relapse rates remain stubbornly high, with estimates ranging from 40% to 60% (McLellan et al., 2000). While the medicalization of addiction has yielded important insights and increased access to care, it has also entrenched a paradigm that defines addiction largely through symptomatology—namely, the presence or absence of substance use. This use/non-use model dominates clinical diagnosis, funding mechanisms, and treatment metrics. Yet it fails to adequately explain the underlying causes of addiction or to account for why some individuals recover while others relapse repeatedly.
This paper introduces the Critical Existential Theory of Addiction and Recovery (CETAR), a multidisciplinary framework that reframes addiction not as a behavioral or neurochemical condition alone, but as a failure of existential integration—a Critical Existential Failure (CEF). CETAR posits that addiction emerges when individuals are unable to construct or sustain a meaningful worldview, derive stable self-esteem, or mitigate death anxiety through symbolic and cultural participation. Substances, in this context, are not merely chemical reinforcers but existential tools that temporarily resolve deep disruptions in meaning-making and social identity.
The goal of CETAR is not to displace existing models of addiction, but to expand them. Drawing from existential psychology (Frankl, Yalom), Terror Management Theory (Becker; Greenberg et al.), and empirical research on spirituality and recovery, CETAR offers an integrated theory that locates addiction at the intersection of self-esteem, mortality salience, and symbolic meaning. The framework invites a critical reevaluation of how we define addiction, how we measure recovery, and how treatment can be meaningfully structured.
Current paradigms—whether rooted in neuroscience, behaviorism, or cognitive therapy—have struggled to account for the subjective and cultural dimensions of addiction. Although spiritually oriented recovery programs like Alcoholics Anonymous (AA) have long described addiction as a “spiritual malady,” their success has often been dismissed as anecdotal or unscientific. Ironically, many of the elements central to recovery in such frameworks—purpose, humility, community, honesty—are also those most neglected in contemporary addiction science. CETAR argues that these are not peripheral concerns, but central mechanisms.
This theory is timely not only because of the ongoing opioid crisis and the institutional failures of the treatment industry, but also because the existing scientific discourse has become increasingly fragmented. What is needed is not simply better data, but a better conceptual framework that can accommodate the full complexity of addiction as both a clinical condition and a human experience.
CETAR is both a critique and a proposal. It critiques the symptom-focused reductionism that has dominated addiction science and proposes a shift toward existential assessment and recovery strategies rooted in quality of life, mortality salience, and the restoration of symbolic value. This paper lays out the theoretical underpinnings of the CETAR framework, explores its implications for treatment and research, and outlines a path forward for empirical investigation.
In doing so, we aim to re-center addiction studies around the lived experience of the sufferer—not merely as a neurochemical machine or moral failure, but as a person navigating meaning, identity, and mortality. Addiction is not just a matter of what one uses, but of what one cannot live without. CETAR asks not only why people use substances, but what those substances mean—and what might replace them if the existential deficit at the heart of addiction can be addressed.
2. Limitations of Current Models
Mainstream addiction science has largely been dominated by biomedical, behavioral, and cognitive paradigms that define and diagnose addiction through the lens of observable substance use. From the American Medical Association’s 1956 declaration of alcoholism as a disease to the DSM’s evolving criteria, addiction has been progressively codified as a clinical disorder with identifiable symptoms—chief among them, the compulsive use of substances despite negative consequences. This use/non-use paradigm has become the primary framework for clinical assessment, treatment success metrics, and research design.
Yet despite its diagnostic clarity and empirical appeal, the use/non-use model remains deeply inadequate as a theory of addiction. First, it fails to distinguish between qualitatively different types of substance users—those with compulsive, life-disrupting addictions and those whose use is situational, temporary, or culturally normative. As a result, diagnostic tools often blur the boundary between problematic and non-problematic use, conflating addiction with high-intensity or socially unacceptable behavior. This leads to both over-pathologization and under-treatment: some individuals are labeled as “addicts” based on use patterns that would not lead to long-term harm, while others with profound existential disconnection and psychological pain are missed entirely because they happen to be abstinent.
Second, the use/non-use paradigm obscures the mechanisms of both addiction and recovery. Abstinence may correlate with recovery, but it is not synonymous with it. Many individuals maintain abstinence without achieving improved quality of life, while others report transformative change without immediate or complete cessation. By focusing on behavior (use) rather than meaning, motivation, or internal transformation, the model fails to explain why some individuals are able to recover and others are not—despite receiving similar interventions.
Third, addiction science has been shaped and constrained by broader socioeconomic forces, particularly neoliberalism, the pharmaceutical industry, and the treatment-industrial complex. As demand for “evidence-based” treatments has grown—often tied to insurance reimbursements and regulatory frameworks—research has prioritized interventions that are easily measurable, replicable, and fundable. This has resulted in a proliferation of narrowly defined, protocol-driven therapies that emphasize symptom reduction over existential integration. Meanwhile, spiritually oriented recovery communities such as AA, which offer subjective but powerful accounts of change, are dismissed in academic and clinical settings for lacking empirical rigor—even as they remain the most widely utilized and enduring sources of recovery support (Priester et al., 2009).
Critiques of AA and other spiritual programs often rest on a fundamental misunderstanding: that recovery is a behavior rather than a transformation. Critics argue that the success of 12-step groups cannot be empirically separated from “spontaneous remission,” and that their effects are statistically indistinguishable from natural recovery (Dodes, 2014). Yet this critique misframes the issue. If existential, spiritual, or social transformation is a valid mechanism of recovery—as abundant anecdotal and qualitative data suggest—then the inability to separate it from remission in current research designs speaks more to the limitations of those designs than to the irrelevance of spiritual change.
Even the fields of neuroscience and cognitive psychology, which have yielded significant insights into the brain’s response to addictive substances, struggle to account for why certain individuals are vulnerable to addiction in the first place, and how recovery occurs in the absence of medication or behavioral therapy. While brain scans can show the effects of substances on dopamine systems or executive function, they cannot explain the deep existential despair or symbolic alienation that many addicts report prior to using—or the sense of purpose, relief, and belonging they often discover in recovery communities.
Moreover, modern addiction science has largely ignored the existential and cultural dimensions of recovery that have become prominent in adjacent fields. In areas such as gerontology, oncology, and palliative care, quality of life (QOL) is increasingly recognized as a central treatment goal, often assessed through existential indicators such as purpose, autonomy, dignity, and the ability to make meaning out of suffering (La Cour & Hvidt, 2010). It is perplexing that addiction—one of the few diseases where behavior, identity, and meaning are so intimately intertwined—remains so resistant to existential inquiry.
The consequence of this omission is that much of addiction research and treatment is stuck in a reductive loop: measuring a symptom (substance use), prescribing interventions to reduce that symptom, and then using the reduction of that symptom as proof of efficacy. This circular logic has led to the proliferation of interventions that are clinically valid but experientially hollow. Individuals may reduce or stop their substance use, yet continue to live in despair, isolation, or spiritual bankruptcy—states that are neither tracked nor treated under current paradigms.
This reductionism also skews our understanding of relapse. Within the use/non-use framework, relapse is seen as a failure of will, treatment compliance, or behavioral control. CETAR reframes relapse as the predictable result of unresolved Critical Existential Failure—a breakdown in the ability to sustain meaning, self-esteem, and existential coherence. From this perspective, relapse is not a moral or psychological weakness, but a reversion to the only existential coping mechanism the individual has known.
In sum, the dominant models of addiction have produced valuable insights, but they have also created blind spots. The symptom-based paradigm has led to a neglect of the existential, symbolic, and meaning-centered dimensions of addiction and recovery. It has favored short-term, measurable outcomes over long-term existential transformation. And it has marginalized frameworks that do not fit neatly into empiricist methodologies—despite their historical effectiveness and deep alignment with the lived experiences of those in recovery.
CETAR emerges from the conviction that addiction is not merely a problem of behavior or biology, but of existence. To understand and effectively treat addiction, we must look beyond use and abstinence and examine the existential mechanics of self-worth, mortality salience, and symbolic belonging. Only then can we begin to construct a more comprehensive and humane framework for understanding what addiction is—and what recovery might truly require.
3. Theoretical Foundations of CETAR
The Critical Existential Theory of Addiction and Recovery (CETAR) draws upon several interwoven theoretical traditions to conceptualize addiction as a failure of existential integration rather than merely a behavioral or chemical disorder. At its core, CETAR synthesizes three central frameworks: existential psychology, Terror Management Theory (TMT), and the spiritual malady model drawn from recovery cultures like Alcoholics Anonymous (AA). Together, these provide a multidimensional understanding of how meaning, mortality, and self-esteem interact in the genesis and resolution of addiction.
3.1 Existential Psychology and Meaning-Making
Existential psychology views the human being not simply as a biological organism or psychological machine, but as a meaning-seeking creature confronted with the inevitability of suffering, death, and freedom. Viktor Frankl, a key figure in this tradition, famously argued that the search for meaning is the primary motivational force in human life (Frankl, 1946). Unlike the Freudian drive for pleasure or the Adlerian pursuit of power, Frankl believed that human well-being is fundamentally rooted in the capacity to construct and sustain a meaningful worldview.
Addiction, from an existential standpoint, can be understood as a form of pathological adaptation—a compulsive attempt to resolve a chronic failure to derive meaning and purpose. Yalom (1980) emphasized that existential anxiety—particularly the awareness of death, isolation, and meaninglessness—lies at the heart of many psychological disturbances. When individuals are unable to face these realities directly or construct frameworks to mitigate them, they may turn to avoidance strategies, including substance use, to dull existential pain.
This perspective is supported by empirical work showing that recovery is strongly correlated with improvements in quality of life and existential well-being, not just abstinence (Laudet et al., 2006). In this light, substances are not only chemical reinforcers but symbolic tools that momentarily alleviate existential distress by simulating belonging, transcendence, or emotional clarity.
3.2 Terror Management Theory (TMT)
Terror Management Theory (TMT), originally derived from Ernest Becker’s The Denial of Death (1973), provides a social psychological model of how human beings cope with the knowledge of their mortality. Becker argued that the awareness of death, coupled with the drive for meaning, produces a fundamental existential tension: we are symbolic beings who yearn for permanence but are biologically finite. To resolve this tension, humans create cultural worldviews—shared symbolic systems that provide a sense of order, value, and continuity beyond the individual lifespan.
According to TMT, two major mechanisms help buffer individuals from mortality salience (MS)—the conscious or unconscious awareness of one’s own death. These are:
- Self-esteem, which affirms one’s value within a meaningful social and cultural order.
- Cultural worldviews, which provide symbolic immortality through tradition, legacy, or spiritual narratives.
When these buffers are weakened—through trauma, social exclusion, or symbolic incoherence—death anxiety rises, leading to psychological distress and maladaptive coping. Empirical studies have consistently shown that reminders of mortality increase defense of cultural norms, bolster self-esteem-enhancing behaviors, and even influence consumer decisions and political attitudes (Pyszczynski, Greenberg, & Solomon, 1999; Burke et al., 2010).
TMT has only recently begun to be applied to addiction studies. Preliminary findings suggest that individuals with low self-esteem are more likely to use substances to reduce MS, particularly when confronted with existential threat (Wisman et al., 2015). From the CETAR perspective, this supports the hypothesis that addiction emerges when traditional MS buffers—symbolic meaning, cultural inclusion, and self-worth—are damaged or inaccessible.
3.3 The Spiritual Malady: Existential Insight from Recovery Culture
While existential psychology and TMT provide the academic scaffolding for CETAR, its experiential roots lie in the concept of the “spiritual malady” as articulated in recovery communities such as AA. In AA’s foundational text, Alcoholics Anonymous (1939), addiction is described not merely as a chemical dependency but as a deep spiritual disorder characterized by restlessness, irritability, and discontent. These states are not defined in purely psychological terms but as existential crises—feelings of alienation, purposelessness, and emotional discord that precede substance use and persist in its absence.
This model, though often dismissed as unscientific, reflects a striking parallel to existential theories. Like Frankl’s “existential vacuum” or Yalom’s “existential anxiety,” the “spiritual malady” captures the internal collapse of symbolic meaning and the disintegration of coherent identity. From this perspective, addiction is not caused by the substance itself, but by the individual’s relationship to the world—a relationship marked by futility, fear, and loss of self.
The recovery process, therefore, is not just about abstaining from substances but about undergoing a radical existential transformation. This is often described in AA as a “spiritual awakening”—a conversion-like shift in values, perception, and self-understanding that reorients the individual toward meaning and purpose. While such experiences have traditionally been viewed as subjective or anecdotal, they align closely with documented psychological phenomena such as spontaneous remission, cognitive reappraisal, and sudden gains in therapy (Paloutzian et al., 1999; Park, 2005).
CETAR reinterprets the spiritual malady through the lens of existential failure and mortality salience. It proposes that the addict or alcoholic is someone who suffers from Critical Existential Failure (CEF)—a breakdown in their ability to construct meaning, maintain symbolic coherence, and buffer death anxiety through culturally sanctioned avenues. This failure may arise from developmental trauma, disrupted socialization, neurological sensitivity, or environmental factors, but its psychological core is existential dislocation.
3.4 Integrative Synthesis
By integrating existential psychology, TMT, and recovery culture, CETAR provides a comprehensive framework that locates addiction not merely in the brain or behavior, but in the symbolic and cultural structures that shape human life. It understands substances as temporary solutions to existential breakdown—tools that mimic connection, coherence, and self-worth, but ultimately deepen the original wound.
This synthesis yields several key insights:
- Addiction is not primarily about substances, but about meaning. The use of drugs and alcohol is symptomatic of a deeper disruption in symbolic and existential systems.
- Self-esteem and cultural inclusion are protective against addiction, not just psychologically but existentially. When these are lost, death anxiety rises, and the individual becomes vulnerable to maladaptive coping.
- Recovery requires more than abstinence. It necessitates the construction of a new worldview, participation in a meaningful social context, and the development of existential authenticity.
- Relapse reflects unresolved existential tension, not just failed behavioral control. Without sustained efforts to repair the underlying symbolic structure of the self, the return to substance use becomes a return to the only available buffer against MS.
This theoretical foundation sets the stage for the next section, in which we explore how CETAR conceptualizes addiction as a trajectory of existential failure—and how its reversal becomes the path to recovery.
4. Critical Existential Failure (CEF) as Etiology
At the heart of the Critical Existential Theory of Addiction and Recovery (CETAR) lies the concept of Critical Existential Failure (CEF), which CETAR identifies as the primary etiological factor that distinguishes those prone to addiction from the general population. CEF refers to a fundamental deficit in the individual’s capacity to construct, maintain, and translate symbolic meaning into coherent self-esteem and existential security. Rather than viewing addiction as a disease defined by neurochemical imbalance or behavioral dysregulation, CETAR asserts that addiction arises when the symbolic frameworks that typically shield human beings from mortality salience (MS) and existential anxiety break down or fail to develop.
This section outlines the nature, origins, and mechanisms of CEF, positioning it as the central explanatory construct in addiction etiology.
4.1 Defining Critical Existential Failure
CEF is characterized by three interrelated dysfunctions:
- Inability to derive meaning from adversity – The person cannot integrate suffering, challenge, or trauma into a coherent personal narrative that reinforces self-worth or life purpose.
- Inability to generalize value across time – The individual struggles to conceptualize long-term goals, delayed gratification, or existential continuity beyond immediate emotional states.
- Inability to experience or sustain symbolic self-esteem – The person is either unable to perceive themselves as valuable within their cultural context, or cannot internalize positive regard from others.
Together, these dysfunctions leave the individual vulnerable to rising MS and chronic existential anxiety. In the absence of stable symbolic meaning or intrinsic self-worth, substances function as temporary existential regulators—tools for bypassing failed meaning-making structures and achieving brief respite from mortality awareness and social dislocation.
4.2 Origins of CEF: Developmental and Environmental Pathways
CETAR does not attribute CEF to a single origin, but recognizes it as the potential result of multiple interacting pathways. These include:
- Developmental trauma and inconsistent socialization – When children are raised in environments that are emotionally unpredictable, abusive, or lacking in symbolic reinforcement (e.g., praise, consistency, moral frameworks), they may fail to form a reliable self-concept rooted in meaning and value. This disrupts the development of intrinsic self-esteem and inhibits their ability to translate social cues into existential security.
- Genetic and epigenetic vulnerability – While CETAR is not a biological theory, it recognizes the plausibility of diathesis-stress models in which genetic predispositions interact with early environmental stressors to impair symbolic processing or emotion regulation. Some individuals may be neurologically more susceptible to symbolic incoherence, hypersensitivity to rejection, or MS activation.
- Cultural exclusion and symbolic marginalization – Individuals from marginalized groups—due to race, class, disability, sexual orientation, or other structural factors—may experience chronic invalidation of their symbolic identity. This leads to existential alienation even when their behavioral conformity is high. Simply put, it is possible to appear socially functional while still experiencing profound CEF.
What unites these pathways is not their precise origin, but their effect: a failure to develop the internal structures necessary for transforming social inclusion, cultural meaning, and relational affirmation into existential coherence.
4.3 The Interplay of CEF, Self-Esteem, and Mortality Salience
Terror Management Theory (TMT) provides a compelling mechanism by which CEF leads to addiction. In the TMT model, self-esteem serves as a psychological buffer against mortality salience. When individuals feel valued, seen, and socially affirmed within a cultural worldview, they are protected from the destabilizing awareness of death. Conversely, when self-esteem is low—or when symbolic participation in culture is disrupted—mortality salience becomes chronically activated.
For individuals with CEF, this buffer system is impaired or non-functional. They are either unable to absorb self-worth from cultural participation, or they remain existentially unprotected even when others affirm them. This leads to chronic or recurrent states of existential anxiety, which manifest as restlessness, alienation, discontentment, and despair—states often described by people with addiction long before substance use becomes problematic.
In this context, substance use is not initially about pleasure or escape—it is about coherence. Alcohol and drugs temporarily amplify or simulate the social and symbolic experiences that individuals with CEF cannot reliably access through “normal” interaction. When intoxicated, the person may finally feel connected, worthy, confident, or safe. These states are not merely emotional—they are existential: they restore, albeit temporarily, a sense of alignment with the world.
This explains why individuals with CEF often describe their first experiences with substances in ecstatic, even spiritual terms. For them, substances don’t just numb—they translate. They bridge the gap between the self and the symbolic world, allowing the person to feel meaningfully alive for the first time.
4.4 Symbolic Translation Deficit: The Hidden Mechanism
A critical feature of CEF is what CETAR identifies as a symbolic translation deficit. This refers to the inability of the individual to meaningfully absorb cultural feedback and convert it into a stable sense of personal value. For most people, praise, inclusion, success, or social bonds reinforce the symbolic sense of “mattering” in the world. For those with CEF, such reinforcement often fails to “land.” The person may understand cognitively that they are valued but feel it as hollow or untrue. This creates an internal split between perception and experience.
This symbolic disconnection explains why individuals with CEF often struggle with relationships, work, or community despite apparent success. They may have social roles, achievements, or support, but feel persistently “othered,” invisible, or fraudulent. They may describe life as empty, surreal, or disconnected from any deeper personal significance. In such cases, the person is not suffering from depression per se, but from a form of existential agnosia—an inability to feel the meaning that others can access naturally.
Substances correct this deficit by flooding the symbolic field with immediacy and intensity. Under the influence, meaning is no longer abstract—it is visceral. Connection becomes real. Joy becomes accessible. Love becomes felt. In this sense, substances act as existential prosthetics—stand-ins for a symbolic translation process that has broken down.
4.5 Addiction as CEF in Action
Addiction, within the CETAR model, is not merely a neurobiological compulsion or a learned behavior pattern. It is the repetitive and escalating attempt to repair or bypass existential failure through chemical means. The substance becomes the only reliable translator of meaning, the only effective reducer of MS, and the only consistent source of symbolic connection.
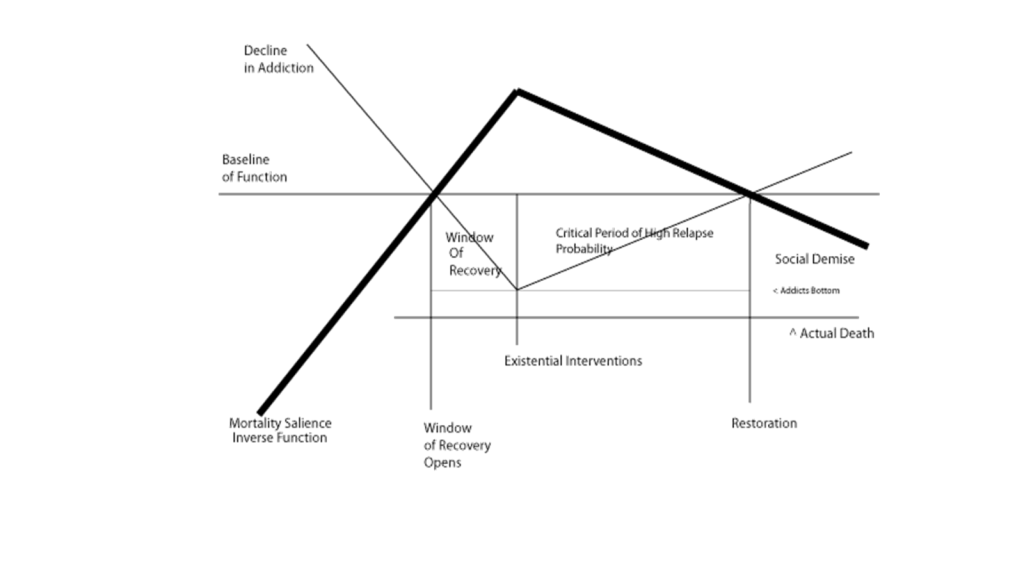
Over time, however, the substance loses its power. As tolerance increases and consequences accumulate, the very act of using begins to increase MS rather than relieve it. Health deteriorates. Relationships collapse. Social roles vanish. The person begins to face literal or symbolic death—homelessness, incarceration, ostracization. The buffer is broken, and the original failure re-emerges, now magnified.
Yet paradoxically, it is in this moment—the moment of existential crisis—that a window for recovery opens. The substance no longer works. The person is exposed to raw mortality salience, and for a brief period, they may be open to new symbolic frameworks that can restore existential coherence. This mechanism, which CETAR will explore in the following sections, underlies the “moment of clarity” described in recovery narratives.
4.6 The Need for a New Etiological Lens
CEF is not meant to replace neurobiological or psychological theories of addiction, but to deepen them. It offers a why to complement the how. It explains not only the development of compulsive use but also the phenomenological experience of addiction—the feeling of being spiritually bankrupt, disconnected, or doomed. These experiences are not metaphors; they are descriptions of existential reality.
By centering addiction on existential failure rather than substance behavior, CETAR shifts the question from what someone uses to why they must use in order to exist. This reframing has profound implications for treatment, which we will now explore by examining the mechanics of recovery through shifts in mortality salience and the reconstruction of meaning.
5. Mechanism of Addiction and Recovery in CETAR
If Critical Existential Failure (CEF) is the etiological root of addiction, then the mechanisms of addiction and recovery must be understood in terms of existential regulation. The CETAR framework proposes that addiction is not merely the result of exposure to substances, nor is recovery merely the cessation of their use. Rather, addiction is a maladaptive coping strategy that emerges from an inability to construct meaning and manage mortality salience (MS), while recovery is a shift in existential orientation—often triggered by moments of crisis or clarity—that re-establishes symbolic coherence and self-esteem through principled action, connection, and authentic meaning-making.
This section maps out the trajectory of addiction as a cycle of temporary MS relief followed by collapse, and outlines how recovery unfolds when new existential structures become viable.
5.1 Addiction as Existential Regulation
From the CETAR perspective, the addictive process is better understood not as compulsive pleasure-seeking or faulty decision-making, but as an ongoing attempt to regulate existential distress. Individuals suffering from CEF lack reliable access to symbolic self-esteem and meaning. As a result, they experience chronically elevated MS—either consciously (as anxiety, dread, despair) or unconsciously (as restlessness, impulsivity, or emotional dysregulation).
Substances enter this context not as hedonistic agents, but as existential anesthetics and symbolic amplifiers. In the early stages of use, alcohol and drugs provide intensely meaningful experiences—euphoria, connection, belonging, transcendence—that temporarily resolve the existential void. These substances act as interpretive tools that allow the user to feel emotionally synchronized with their world, often for the first time.
The addict or alcoholic, then, is not merely intoxicated; they are aligned. Their internal sense of symbolic detachment and social alienation is suspended. Life appears coherent, vivid, and bearable.
Yet as tolerance develops and external consequences mount, the original relief becomes harder to access. MS begins to rise again, but now the substance—once the antidote—becomes part of the problem. Health problems, broken relationships, and social decline increase mortality salience, and the user begins to face both literal and symbolic death. The substance that once relieved MS now exacerbates it. A crisis emerges.
5.2 The Mortality Salience Shift and the “Window to Recovery”
CETAR identifies a key moment in the trajectory of addiction: the MS shift, or what recovery cultures refer to as a “moment of clarity.” This is a point at which the substance can no longer resolve existential anxiety, and the individual becomes acutely aware of the mortality threat—physical, emotional, or social—that their addiction entails.
The MS shift occurs when three conditions converge:
- Rising self-awareness of existential threat – The addict internalizes the reality of death (literal or social), often triggered by a crisis such as a health scare, arrest, or loss of a loved one.
- Recognition of the substance as the problem – The individual no longer believes that their drug of choice will alleviate their suffering, and may begin to see it as a source of despair.
- Perceived insufficiency of personal resources – The addict acknowledges that they cannot resolve this crisis with their current coping strategies or worldview.
These shifts may be sudden or gradual, and they often resemble conversion experiences in religious literature—sudden reorientations of perception and values. In this moment, the individual becomes open to new existential frameworks, because the old ones have failed completely.
It is at this point that recovery becomes possible—not because the person has become rational or compliant, but because their existential system is in collapse, and they are willing to reconstruct it from the ground up.
5.3 Existential Reorientation Through Principled Action
What replaces the substance as a means of existential regulation? CETAR argues that recovery requires the development of authentic, socially embedded, and principled frameworks through which the individual can reconstruct symbolic meaning and self-worth. This typically involves:
- Engagement with a value system larger than the self – Often spiritual or community-based, but not necessarily religious.
- Commitment to principled action – Honesty, service, humility, accountability—values that both restore self-esteem and foster social inclusion.
- Acceptance of existential limits – Including mortality, imperfection, and suffering. This acceptance marks the shift from existential inauthenticity (denial, avoidance) to authenticity (engagement, resilience).
The 12-step model exemplifies this process. Steps such as admitting powerlessness, making amends, and helping others are not moral tasks—they are existential exercises. They recalibrate the individual’s symbolic world, allowing for new forms of meaning-making that are socially validated and personally coherent.
Importantly, this transformation is not simply a change in beliefs. It is a shift in being—an existential restructuring that enables the individual to find value in life without the aid of substances. Abstinence becomes a side effect of this transformation, not its goal.
5.4 Existential Authenticity and the Stabilization of Recovery
Long-term recovery, in the CETAR model, depends on the stabilization of existential authenticity. Borrowing from existential psychology, authenticity refers to the individual’s ability to live in accordance with their values, accept their limitations, and remain engaged with the reality of human suffering without denial or flight.
This does not mean perpetual emotional serenity. Rather, it means the person is no longer seeking to escape life, but to live it on meaningful terms. They have developed symbolic structures—whether through community, spirituality, creative work, or service—that buffer MS and sustain self-esteem.
Critically, this authenticity must be embodied. Passive belief in values is insufficient. It is action, embedded in social and symbolic systems, that produces transformation. This is why recovery programs emphasize behaviors: attending meetings, making amends, sponsoring others. These are existential interventions, not therapeutic rituals.
When recovery falters, it is often because existential authenticity has not fully taken hold. The individual may be abstinent but still existentially untethered—lacking coherence, purpose, or social affirmation. In such cases, MS gradually rises again, and without a reliable existential framework, the individual is vulnerable to relapse.
5.5 Relapse as Existential Regression
Within CETAR, relapse is not a failure of willpower or a breakdown of behavioral control. It is a regression to the only known existential buffer. When principled action and meaning-making falter, and when social support wanes or loses salience, MS begins to rise. For individuals with CEF, the familiar response is to return to substances, which—despite their diminishing efficacy—remain the most reliable method they have ever known to re-establish coherence.
This understanding of relapse has profound implications. It suggests that preventing relapse is not about increasing behavioral compliance, but about deepening existential engagement. It calls for more than coping skills—it calls for meaning.
Relapse, then, should be viewed as a crisis of symbolic identity, not merely a behavioral event. Interventions must address the individual’s social embeddedness, access to principled action, and capacity for symbolic self-translation. Without these, abstinence will remain tenuous, regardless of therapeutic effort.
5.6 Recovery as Existential Mastery, Not Abstinence
Finally, CETAR proposes that successful recovery is best understood not as a state of non-use, but as a state of existential mastery. This means:
- The individual can navigate MS without fleeing into substances.
- Self-esteem is stable, culturally grounded, and internally reinforced.
- Life is experienced as meaningful, even amidst suffering.
- Symbolic coherence is sustained through principled, social action.
Such individuals are not “cured” in the traditional sense. Rather, they have developed an existential immune system robust enough to face life on its own terms. They do not merely abstain—they belong, act, and matter in ways that are felt, not just known.
This reframing opens the door to new models of care, new assessment tools, and new clinical strategies. It also calls for a broader cultural reevaluation of what it means to heal—not just from addiction, but from existential dislocation.
In the next section, we will explore the practical and empirical implications of CETAR for clinical practice and addiction science.
6. Implications for Treatment and Research
If the Critical Existential Theory of Addiction and Recovery (CETAR) provides a more comprehensive understanding of addiction as rooted in existential failure rather than substance use, then it necessarily demands a rethinking of how addiction is measured, treated, and studied. CETAR challenges the clinical status quo by asserting that recovery must be assessed through existential and quality-of-life frameworks, and not merely by counting days of abstinence or cataloging symptoms.
This section explores CETAR’s implications across three core domains: (1) clinical treatment and intervention design, (2) measurement and assessment reform, and (3) empirical research directions.
6.1 Clinical Treatment: From Symptom Suppression to Existential Repair
In the current treatment landscape, many modalities emphasize symptom reduction, compliance, and behavioral regulation. While these approaches can be helpful in managing acute risk, CETAR argues that they often fail to address the deeper existential roots of addiction. Without interventions that engage meaning-making, symbolic coherence, and authentic social integration, many individuals achieve only “functional abstinence”—they stop using substances, but remain psychologically, socially, and spiritually adrift.
CETAR reframes treatment not as symptom suppression, but as existential repair. The goal is to help the individual rebuild a worldview in which they:
- Feel fundamentally valued and visible within their social environment;
- Can translate adversity into purpose, identity, and resilience;
- Develop authentic, principled behaviors that anchor self-esteem and affirm social worth;
- Learn to engage mortality salience without regressing into substance use.
Therapists and counselors, therefore, must become facilitators of existential realignment. Practices such as motivational interviewing, narrative therapy, logotherapy, existential psychotherapy, and structured spiritual mentorship are especially well-suited for these aims. But CETAR also calls for a more widespread integration of spiritual, cultural, and philosophical dialogue into clinical settings—not as adjuncts, but as central mechanisms of healing.
Additionally, treatment must focus on catalyzing mortality salience shifts (MS shifts) in ways that are ethically sound and psychologically constructive. Therapeutic confrontation, reflective writing, group disclosure, grief work, and guided readings (e.g., Becker’s The Denial of Death) can all serve to bring existential concerns into the foreground—creating conditions for insight, transformation, and recommitment.
6.2 Measurement and Assessment: Moving Beyond the Use/Non-Use Paradigm
One of CETAR’s most urgent critiques is that addiction science lacks adequate tools for measuring the core dynamics of addiction and recovery. Clinical assessments remain anchored in the use/non-use paradigm, emphasizing frequency of use, cravings, triggers, or DSM diagnostic thresholds. These measures, while useful for clinical triage and insurance billing, obscure the internal, symbolic, and existential processes that determine whether a person is actually recovering.
CETAR calls for a new generation of existential quality-of-life (QOL) measures designed specifically for addiction contexts. These tools should:
- Evaluate the individual’s capacity to derive meaning from their life experiences;
- Assess existential authenticity, such as the alignment between values and behavior;
- Measure the ability to translate social cues into stable self-esteem;
- Identify persistent experiences of mortality salience, symbolic isolation, or ontological insecurity.
Such instruments could be adapted from existing QOL scales used in oncology, geriatrics, or palliative care (e.g., the McGill Quality of Life Questionnaire), but would need to be tailored to addiction-specific concerns. Alternatively, a new instrument could be developed from the ground up, using thematic analysis of subjective narratives (e.g., “restless, irritable, and discontent”) to identify key existential markers.
Importantly, CETAR proposes that such assessments should not rely on substance use data. In fact, a valid CETAR-informed instrument should be able to distinguish between individuals with high-functioning abstinence and those with low-functioning abstinence, regardless of whether substance use is present. Similarly, it should identify at-risk individuals whose existential dislocation makes them vulnerable to future substance misuse—even if they currently use sparingly or not at all.
6.3 Research Implications: Testing CETAR’s Hypotheses
CETAR’s theoretical model makes several testable hypotheses that could guide future empirical research:
- Individuals with high existential coherence (measured via symbolic meaning, social belonging, and intrinsic self-esteem) will show lower rates of problematic substance use, even when controlling for demographics, trauma history, and access to care.
- Substance use is significantly correlated with mortality salience activation, especially in individuals with low self-esteem and symbolic disconnection (e.g., marginalized populations, individuals with trauma histories, etc.).
- Recovery trajectories are best predicted by changes in existential variables, not by substance use patterns alone. For example, individuals who report improved meaning-in-life scores may maintain abstinence even in high-risk environments, while those with persistent existential distress relapse despite behavioral interventions.
- Therapeutic interventions that target mortality salience, symbolic meaning, and social value restoration (e.g., logotherapy, values-based interventions, recovery communities rooted in spiritual or moral frameworks) will outperform traditional behavioral interventions in long-term recovery outcomes, especially among those with histories of trauma, alienation, or chronic relapse.
In methodological terms, CETAR encourages the use of mixed methods research. Qualitative narrative analysis can identify existential themes, while quantitative tools can test correlations between meaning, MS, and recovery outcomes. Experimental designs might also manipulate MS (as in TMT studies) and observe changes in substance use intention or coping responses across different self-esteem levels.
Additionally, longitudinal research can explore how existential factors evolve over time in people in recovery. Do early gains in meaning-making predict stable recovery? Do existential disruptions (e.g., loss of a loved one, moral failure, spiritual crisis) forecast relapse more reliably than behavioral markers? These are empirical questions that CETAR makes visible.
6.4 Redefining Recovery and Relapse
Perhaps most radically, CETAR calls for a cultural and clinical redefinition of recovery. Rather than equating it with abstinence or “sobriety,” recovery should be understood as the restoration of existential coherence. The recovering person is one who:
- Experiences life as meaningful;
- Maintains symbolic and social inclusion;
- Has developed stable, intrinsic self-esteem;
- Can face mortality salience without fleeing into self-destruction.
Similarly, CETAR redefines relapse as not simply a return to use, but as a collapse of existential structures. A person may relapse months before they pick up a drink or drug—when they lose their sense of purpose, abandon principled action, or become symbolically isolated. Recognizing relapse as an existential process can shift treatment goals from reactive management to proactive meaning restoration.
6.5 Portability and Broader Relevance
While CETAR is focused on addiction, its underlying framework has applications beyond substance use. The interplay between mortality salience, self-esteem, and symbolic meaning is relevant to a range of psychological phenomena, including depression, PTSD, chronic illness, and suicidality. In this way, CETAR may serve as a foundation for a broader existential psychology that reconnects clinical science with the lived experience of being human.
In the final section, we synthesize the CETAR model and revisit its core contributions, offering a brief conclusion and roadmap for continued theoretical and empirical development.
7. Conclusion
The Critical Existential Theory of Addiction and Recovery (CETAR) offers a new paradigm for understanding addiction—not as a disorder defined by the presence of substance use, but as a condition rooted in Critical Existential Failure (CEF). CETAR reframes addiction as a collapse of the human ability to construct symbolic meaning, sustain self-esteem, and mitigate mortality salience (MS) through social and cultural participation. In this view, substance use is not the disease itself, but the symptom of a deeper existential dislocation.
CETAR integrates insights from existential psychology, Terror Management Theory (TMT), and long-standing recovery traditions—particularly those that emphasize spiritual transformation and principled action. Where dominant paradigms in addiction science focus on behavior and biology, CETAR foregrounds the lived experience of the addict: the feeling of being disconnected from meaning, of existing without symbolic validation, and of using substances as the only accessible form of existential coherence.
In doing so, CETAR challenges the use/non-use paradigm that undergirds current diagnostic and treatment models. It questions the utility of abstinence as the sole metric of recovery and suggests that without addressing the existential roots of addiction, even the best-intentioned interventions may fail. Conversely, CETAR helps explain why spiritually centered recovery communities like Alcoholics Anonymous, though often dismissed as unscientific, continue to provide durable recovery for millions: because they address meaning, mortality, and identity where formal systems often cannot.
The implications of CETAR are far-reaching. Clinically, it calls for interventions that facilitate existential transformation—helping individuals reconstruct symbolic meaning, engage in principled action, and restore authentic belonging. In terms of research, it proposes the development of new assessment tools that measure quality of life, existential authenticity, and mortality salience as primary indicators of addiction and recovery. Conceptually, it invites addiction science to reengage with the broader human questions that addiction so vividly exposes: What makes life meaningful? How do we face death? What does it mean to belong?
CETAR does not reject empirical science—it calls for its expansion. It does not dismiss pharmacological or behavioral interventions—it insists they be integrated within a more comprehensive understanding of what recovery actually entails. Addiction is not merely about what people consume—it is about what people are missing, and what they are trying, however unsuccessfully, to restore.
Ultimately, CETAR asks us to see the addict not as a malfunctioning brain or deviant actor, but as a person in existential crisis. And it asks us to reimagine recovery not as abstinence, but as existential repair. If addiction arises when symbolic systems collapse, recovery begins when meaning returns.
References
Adamson, T. A., & Adekunle, D. A. (2011). Structured relapse prevention in psychostimulant dependence: A pilot study of its efficacy in a Nigerian cohort. African Journal of Psychiatry, 14(3), 208–211. https://doi.org/10.4314/ajpsy.v14i3.3
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). https://doi.org/10.1176/appi.books.9780890425596
Baumeister, R. F., DeWall, C. N., Ciarocco, N. J., & Twenge, J. M. (2005). Social exclusion impairs self-regulation. Journal of Personality and Social Psychology, 88(4), 589–604. https://doi.org/10.1037/0022-3514.88.4.589
Becker, E. (1973). The denial of death. Free Press.
Becker, E. (1962). The birth and death of meaning. Free Press.
Biello, D. (2007). Searching for God in the brain. Scientific American Mind. https://www.scientificamerican.com/article/searching-for-god-in-the-brain/
Burke, B. L., Martens, A., & Faucher, E. H. (2010). Two decades of terror management theory: A meta-analysis of mortality salience research. Personality and Social Psychology Review, 14(2), 155–195. https://doi.org/10.1177/1088868309352321
Carmody, J. (2013). The art of existential therapy: Creativity, love, and healing. Routledge.
Cleary, M., Walter, G., & Hungerford, C. (2014). Recovery and humility. Issues in Mental Health Nursing, 35(10), 769–771. https://doi.org/10.3109/01612840.2014.899983
Csikszentmihalyi, M., & Beattie, O. (1979). Life themes: A theoretical and empirical model of psychological development. New Ideas in Psychology, 1(1), 21–44. https://doi.org/10.1016/0732-118X(79)90014-6
Dodes, L. (2014). The sober truth: Debunking the bad science behind 12-step programs and the rehab industry. Beacon Press.
Frankl, V. E. (1946). Man’s search for meaning. Beacon Press.
Frankl, V. E. (1969). The will to meaning: Foundations and applications of logotherapy. World Publishing.
Galanter, M. (2007). Spirituality and recovery in 12-step programs: An empirical model. Journal of Substance Abuse Treatment, 33(3), 265–272. https://doi.org/10.1016/j.jsat.2007.04.016
Halloran, M. J., & Kashima, E. S. (2004). Social identity and morality in cultural worldview defense and self-esteem threat. Personality and Social Psychology Bulletin, 30(12), 1610–1621. https://doi.org/10.1177/0146167204271182
Harter, S., Waters, P., Whitesell, N. R., & Kastelic, D. (2005). Lack of voice as a manifestation of false self-behavior among adolescents: The school setting as a stage upon which the drama of authenticity is enacted. Educational Psychologist, 30(3), 153–173.
Heather, N. (1998). A conceptual framework for explaining drug addiction. Journal of Psychopharmacology, 12(1), 3–7. https://doi.org/10.1177/026988119801200102
Hopson, M. H., & Beaird-Spiller, D. (1995). Religiousness and spirituality: Can they promote recovery from substance abuse? Counseling and Values, 39(3), 194–200.
Horvath, A. T., & Yeterian, J. D. (2012). SMART Recovery: Self-help for substance use disorders. Journal of Groups in Addiction & Recovery, 7(2–4), 102–117. https://doi.org/10.1080/1556035X.2012.705713
Isbell, H., & White, W. L. (1953). Narcotic addiction and its treatment. Public Health Reports, 68(9), 873–884.
Jonas, E., Kayser, D. N., Sullivan, D., & Greenberg, J. (2008). Mirror, mirror on the wall, I am my enemy after all. Journal of Personality and Social Psychology, 95(2), 263–278. https://doi.org/10.1037/0022-3514.95.2.263
Kurtz, E. (1982). Why A.A. works: The intellectual significance of Alcoholics Anonymous. Journal of Studies on Alcohol, 43(1), 38–80.
La Cour, P., & Hvidt, N. C. (2010). Research on meaning-making and health in secular society: Secular, spiritual and religious existential orientations. Social Science & Medicine, 71(7), 1292–1299. https://doi.org/10.1016/j.socscimed.2010.06.024
Laudet, A. B. (2011). The case for considering quality of life in addiction research and clinical practice. Addiction Science & Clinical Practice, 6(1), 44–55.
Laudet, A. B., Morgen, K., & White, W. L. (2006). The role of social supports, spirituality, religiousness, life meaning and affiliation with 12-step fellowships in quality of life satisfaction among individuals in recovery from alcohol and drug problems. Alcoholism Treatment Quarterly, 24(1–2), 33–73. https://doi.org/10.1300/J020v24n01_04
Lewinsohn, P. M., Joiner, T. E., & Rohde, P. (2001). Evaluation of the hopelessness theory of depression: Predicting first onset of depression. Journal of Abnormal Psychology, 110(2), 203–212.
Lillenfeld, S. O., & Arkowitz, H. (2011). Does Alcoholics Anonymous work? Scientific American Mind, 22(6), 62–63.
Mate, G. (2008). In the realm of hungry ghosts: Close encounters with addiction. Knopf Canada.
McGue, M. (1999). The behavioral genetics of alcoholism. Current Directions in Psychological Science, 8(4), 109–115. https://doi.org/10.1111/1467-8721.00026
McLellan, A. T., Lewis, D. C., O’Brien, C. P., & Kleber, H. D. (2000). Drug dependence, a chronic medical illness: Implications for treatment, insurance, and outcomes evaluation. JAMA, 284(13), 1689–1695. https://doi.org/10.1001/jama.284.13.1689
Minnick, F. (1997). Spirituality and chemical dependency: A treatment perspective. Haworth Press.
Morse, R. M., & Flavin, D. K. (1992). The definition of alcoholism. JAMA, 268(8), 1012–1014. https://doi.org/10.1001/jama.1992.03490080086030
Paloutzian, R. F. (1999). Spiritual conversion and transformation: A meaning-system analysis. In R. W. Hood Jr. (Ed.), Dimensions of Mystical Experiences (pp. 271–281). Brill.
Pargament, K. I., Desai, K. M., & McConnell, K. M. (2004). Spirituality: A pathway to posttraumatic growth or decline? In P. A. Linley & S. Joseph (Eds.), Positive psychology in practice (pp. 121–139). Wiley.
Park, C. L. (2005). Religion and meaning. Psychology of Religion and Spirituality, 1(1), 4–14.
Priester, M. A., et al. (2009). Treatment modality preferences among individuals with co-occurring substance use and mental disorders. Substance Abuse Treatment, Prevention, and Policy, 4(1), 1–11.
Pyszczynski, T., Greenberg, J., & Solomon, S. (1999). A dual-process model of defense against conscious and unconscious death-related thoughts. Psychological Review, 106(4), 835–845.
Reker, G. T., & Chamberlain, K. (1999). Exploring existential meaning: Optimizing human development across the life span. Thousand Oaks: Sage Publications.
Scimecca, J. A. (1979). The sociological paradigm of meaning. Sociological Analysis, 40(4), 295–303.
Solomon, S., Greenberg, J., & Pyszczynski, T. (2000). Pride and prejudice: Fear of death and social behavior. Current Directions in Psychological Science, 9(6), 200–204.
Tarter, R. E. (1988). Are there inherited behavioral traits that predispose to substance abuse? Journal of Consulting and Clinical Psychology, 56(2), 189–196.
Toft, A. (2000). Spirituality as a component of addiction treatment. Journal of Substance Abuse Treatment, 19(4), 363–367. https://doi.org/10.1016/S0740-5472(00)00133-8
Ullman, C. (2013). The transformed self: The psychology of religious conversion. Springer.
White, W. L. (1998). Slaying the dragon: The history of addiction treatment and recovery in America. Chestnut Health Systems.
White, W. L. (2007). Addiction recovery: Its definition and conceptual boundaries. Journal of Substance Abuse Treatment, 33(3), 229–241. https://doi.org/10.1016/j.jsat.2007.04.015
Wilson, B. (1939). Alcoholics Anonymous: The story of how more than one hundred men have recovered from alcoholism. Alcoholics Anonymous World Services.
Wisman, A., Heflick, N. A., & Goldenberg, J. L. (2015). The great escape: The role of self-esteem and self-related cognition in terror management. Journal of Personality and Social Psychology, 108(4), 737–750. https://doi.org/10.1037/pspp0000017
