
The Wall Street Journal recently ran a commentary arguing that “Not Everything is Healthcare.”
Health insurers like UnitedHealthcare, Centene and Humana have devoted billions of dollars in the past decade to building new “affordable housing.” They’re also spending heavily on nutrition programs and local community resources. No, the insurance industry hasn’t suddenly begun emphasizing philanthropy over profit. Rather, it is responding to a recent, concerted shift in public policy toward fostering investment in what are commonly called social determinants of health.
The commentary goes on to question the rigor of the evidence, report weak effects, and argue that research and advocacy have integrity problems—”Research on this subject is entwined with advocacy, subject to financial conflicts of interest and often politically motivated.”
The author frames the whole issue in a pretty damning manner. It’s biased, and appears to want to throw the baby out with the bathwater, but it does raise some important questions.
This is important to me because, before I ever heard the term Social Determinants of Health (SDOH), the best addiction treatment programs were addressing SDOH in ways that were effective and unique.
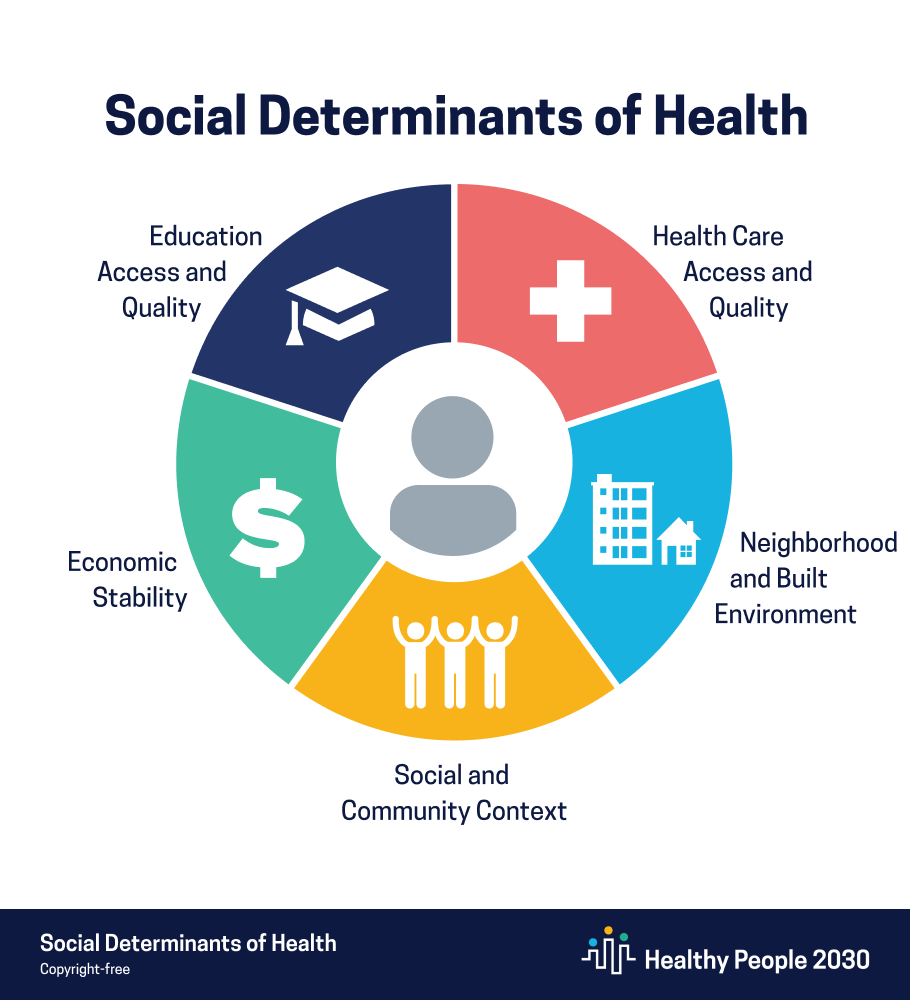
Social determinants of health are defined as the conditions in the environments where people are born, live, learn, work, play, worship, and age that affect a wide range of health, functioning, and quality-of-life outcomes and risks. The idea is that medical care and genetics are important predictors health outcomes, but so are their social, economic, and environmental conditions.
The best treatment programs I referenced provided primary treatment in outpatient and residential settings but also helped clients develop new social support networks, provided family education and counseling, connected with recovery-supportive housing, obtained recovery-supportive (or, at least, congruent) employment, and provided supported pathways to education.
Many people with addiction didn’t need all of these interventions. Others, due to a combination of problem severity, individual factors, and environmental factors, needed these additional supports to recovery initiation and maintenance.
William White, building on the natural recovery work of Cloud & Granfield, attributed these differences, at least in part, to recovery capital (RC). He defined recovery capital as “the breadth and depth of internal and external resources that can be drawn upon to initiate and sustain recovery from severe AOD problems” and identified 3 types: personal capital, family/social capital, and community capital.
Now, SDOH and RC are not identical, but there is a lot of conceptual and practical overlap. The concept is intuitive and rooted in front-line experience. In the case of medical care, a patient with high cholesterol and blood pressure is more likely to make changes in diet and physical activity if they have a life that provides money, time, transportation, access to markets with healthy options, and walkable communities. Whereas, someone with little free-time, in a food desert, and unsafe neighborhoods is less likely to make those lifestyle changes. At the intersection of addiction and medical care, I’ve seen countless addiction patients make significant improvements in their management of problems like diabetes because they had a place to store the insulin, help getting their insulin, and living with people who notice if they seem off and remind them to test their blood sugar and take their insulin.
The impact of these kinds of factors might be thought of as practice-based evidence before it became an evidence-based practice.
So… I have an impulse to push back on the WSJ commentary. It is biased (Do we really need to accuse people of bad motives? Just critique the model and practices) and full of straw men (How many people believe everything is healthcare?), but there are legitimate questions about who will benefit most from addressing SDOH, how best to address them, who should be responsible for them, and what we can reasonably expect. The nature and categories for determinants also call for humility. The downstream effects of these problems are often difficult to address, especially when there are multiple problems interacting and compounding problems.
Medical systems are being required to screen for SDOH. This is a good thing. Providers should be aware of factors that will influence their patients’ outcomes. However, most of those SDOH needs are likely to be best addressed in the community.
Along the lines of my recent post on the loss of trust making programs and models vulnerable, rather than attempting to stifle criticism, it probably makes sense to stop and inventory whether there are frames, advocacy, and applications that make the model more vulnerable. For example, are we over-diagnosing the problem(s), over-extending the conceptual boundaries, acknowledging that we have a lot to learn about effectively addressing SDOH, and what return on investment to expect with what problem and what patient population? A lot of good ideas have suffered because experts and institutions, for whatever reason, overextended them, over-promised outcomes, and got high on their own supply.

majestic! 43 2025 Revisiting William White: We Need More Recovery Custodians and Fewer Recovery Rock Stars (2020) astonishing
LikeLike