
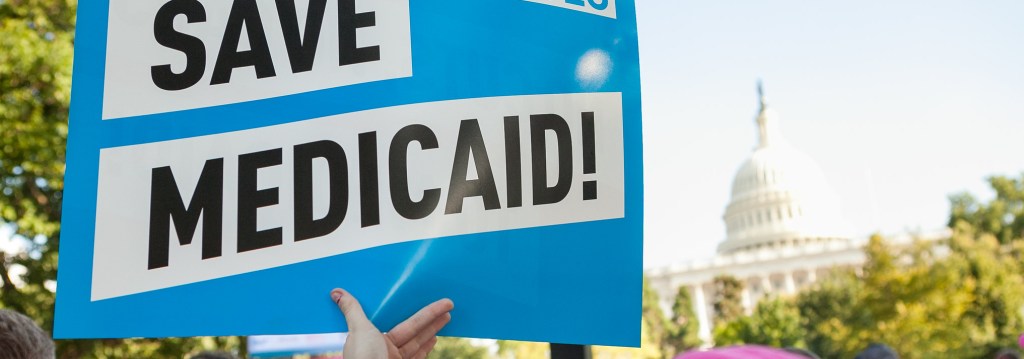
The last few months have been pretty distressing for those of us who care about people with addiction, their access to treatment, as well as the welfare of their families and communities.
- There are credible threats to cut Medicaid funding, which is estimated to fund 30-40% of all substance use disorder treatment in the US.
- The federal freeze on grants is currently stalled in the courts, but the implications for the federal Substance Use Prevention, Treatment, and Recovery Services Block Grant (SUBG) are unclear. The block grant is estimated to fund 20-25% of all substance use disorder treatment in the US.
- SAMHSA staff have been cut by around 10%, and there is an effort to increase those staff cuts to around 50%. I’m told that the Office of Recovery has already had around half of its staff terminated.
- Plus, cuts in research funding and the downstream scarcity in state and local government dollars to respond to alcohol and other drug problems.
I’ve been thinking a lot about how we got here. This is one part of a much larger political and cultural story, but it’s a part I care a lot about. I’m not suggesting that alcohol and other drugs (AOD) problems drove the direction of federal elections and federal policy, but there may be some important ways our responses to AOD problems represent a microcosm of our larger issues.
I believe a driving issue in much of the current disruption is low institutional trust in the addiction/recovery space (and nearly everywhere else).
Why might there be low levels of trust in institutions and reporting in this space? Allow me to digress for a moment.
In last Sunday’s NYT, Zeynep Tufecki described the effort to squelch lab leak theories about the origins of the COVID pandemic.
It’s not hard to imagine how the attempt to squelch legitimate debate might have started. Some of the loudest proponents of the lab leak theory weren’t just earnestly making inquiries; they were acting in terrible faith, using the debate over pandemic origins to attack legitimate, beneficial science, to inflame public opinion, to get attention. For scientists and public health officials, circling the wagons and vilifying anyone who dared to dissent might have seemed like a reasonable defense strategy.
That’s also why it might be tempting for those officials or the organizations they represent to avoid looking too closely at mistakes they made, at the ways that, while trying to do such a hard job, they might have withheld relevant information and even misled the public. Such self-scrutiny is especially uncomfortable now, as an unvaccinated child has died of measles and anti-vaccine nonsense is being pumped out by the top of the federal government. But a clumsy, misguided effort like this didn’t just fail; it backfired. These half-truths and strategic deceptions made it easier for people with the worst motives to appear trustworthy while discrediting important institutions where many earnestly labor in the public interest.
Zeynep Tufekci. (2025, March 16). Opinion | We Were Badly Misled About Covid. Nytimes.com; The New York Times.
She describes how scientists said one thing in public and the opposite in private while using their authority to paint anyone who questioned their narrative as conspiracy theorists.
Note that she acknowledges many of the lab leak theorists were acting in bad faith and spreading misinformation. However, a guilt-by-association strategy was deployed to discredit anyone who asked the wrong questions or challenged their authority.
Why focus on institutions rather than individuals? A quote from Yuval Levin comes to mind.
“We trust an institution when it seems to have an ethic that makes the people within it more trustworthy,” explains Levin. “However, we lose faith in an institution when we no longer believe that it plays that kind of ethical or formative role shaping the people within it to be trustworthy.”
Yuval Levin Explains the Importance of Institutional Trust and Reform | UMD School of Public Policy. (2021, February 25)
While we’re on this COVID tangent, a recent study examined social media activity to better understand why people mistrust vaccines and public health messaging. STAT describes the findings this way:
Communities facing systemic neglect often have little reason to trust public institutions. For decades, many of these areas have endured underfunded schools, limited economic opportunities, and subpar health care. When institutions fail to deliver basic services, skepticism becomes the default. Vaccine mandates, framed as public health necessities, can appear to these communities like just another demand from distant authorities who have long ignored their needs.
This distrust is not limited to one demographic, either. While rural white working-class communities often dominate discussions about vaccine hesitancy, marginalized communities of color — who have faced long-standing disparities in health care access — also report lower vaccination rates. Across these groups, the common thread is a shared experience of exclusion and institutional failure. When public health campaigns frame vaccinations as a moral obligation or use shame as a tactic, they only deepen the divide.
Misinformation is not the main reason for vaccine hesitancy | STAT. (2025, March 14).
In the original paper, the authors offer an analysis of the processes involved in vaccine hesitancy:
The moral foundations theory can illuminate our findings regarding the vaccination hesitant community [92]. The theory suggests that people primarily rely on moral intuitions shaped by socio-psychological factors to make political judgments, then they justify their judgments with strategic reasoning [92]. Some Twitter users’ attitudes toward vaccines may have been shaped by emotions and gut-level feelings, leading to distrust of institutions that underlies vaccine hesitancy. Research has used moral foundations theory to analyze communication patterns and discursive elements in COVID-related social media content [93, 94]. Our findings regarding the spurious relationship between a solitary socio-economic parameter and vaccine hesitancy as well as the indiscriminate use of different topics may support this idea. This distrust may stem from a heightened moral preference expressed through a series of ad-hoc hypotheses, as classified as diverse vaccine-hesitant themes in our study [95].
Ayaz, H., Celik, M. H., Koytak, H. Z., & Yanik, I. E. (2024). Exploring vaccine hesitancy in digital public discourse: From tribal polarization to socio-economic disparities. PloS one, 19(11), e0308122. https://doi.org/10.1371/journal.pone.0308122
This is an interesting and possibly illuminating description of the process and activation of moral, emotional, and cognitive responses to vaccines and public health messaging.
What’s just as interesting is that the authors don’t seem to consider the ways moral foundations theory’s understanding of moral impulses might explain the reactions of public health professionals and other experts when interacting with the public.
Tufekci’s column could suggest that experts may have their own impulses and intuitions that create the conditions for power struggles with interlocutors, asserting dominance, and straying from scientific humility. Further, as the paper described, there may be patterns of post hoc reasoning to support those intuitions. Again, Yuval Levin comes to mind:
Greater public faith in elite institutions requires evidence of restraint, not just of competence
Yuval Levin (2024) The Trust Trap | SAPIR Journal.
The NYT’s The Daily podcast posted an interview with the authors of a new book looking back at the public health responses to the COVID pandemic, specifically the effectiveness of the restrictions and the processes that led to their establishment and maintenance. Here’s an introductory summary:
And so the biggest theme that runs through the book, I think, is that these, as we call them, truth-seeking institutions, did not function as well as they should have during COVID. That there was a premature policy consensus. There was an unwillingness to re-examine assumptions. And there was an intolerance of criticism and divergent points of view that emerged fairly quickly in the pandemic, and that hurt us, that hurt our policy responses, that hurt our ability to course correct over the course of the pandemic as we learned more and had greater reason to course correct.
Stephen Macedo from: Barbaro, M. et al. (2025, March 20). Were the Covid Lockdowns Worth It?; The New York Times.
On the social and cultural pressures:
In the quarters that I travel in among academics or on mainstream media, that’s where there seemed to be little questioning. It was almost seen as wrong or immoral to raise questions about whether this was feasible for most of the population.
Frances Lee from: Barbaro, M. et al. (2025, March 20). Were the Covid Lockdowns Worth It?; The New York Times.
On the role of values and limits of science in public health and policy decisions:
But it also should have involved ordinary people in the public, who after all, were being the ones asked to make sacrifices in their own lives, to adopt policies which always involve trade-offs across values, risks. How much are we willing to give up to not visit an elderly relative in the hospital, to not have a funeral, to not be allowed to attend church on Sunday?
These sorts of public questions don’t have scientific answers. They’re value judgments about which ordinary people have a certain expertise about their own lives and what matters to them. And they should have been involved as well, in the deliberation about these measures.
Stephen Macedo from: Barbaro, M. et al. (2025, March 20). Were the Covid Lockdowns Worth It?; The New York Times.
On the effects of controlling information, stifling questions, asserting authority, and failing to acknowledge unknowns:
Barbaro: Do you worry that conspiracy theories will be fueled by what you’re asking people to do here?
Lee: I think conspiracy theories are fueled by not asking these questions. I mean, obviously, there are many conspiracy theories around COVID. The Plandemic, governments took these actions in order to assert more control over us, I mean, that kind of discourse which exists. If government acknowledged these questions and tried to hash them out, yes, some faith might be lost, but also some faith would be gained.
Barbaro, M. et al. (2025, March 20). Were the Covid Lockdowns Worth It?; The New York Times.
During the episode, they played a portion of comments made by Francis Collins, former Director of NIH, in 2023 regarding the focus and limits of public health:
As a guy living inside the Beltway, feeling the sense of crisis, trying to decide what to do in some situation room in the White House with people who had data that was incomplete, we weren’t really thinking about what that would mean to Wilk and his family in Minnesota, a thousand miles away from where the virus was hitting hard. We weren’t really considering the consequences in communities that were not New York City or some other big city. If you’re a public health person and you’re trying to make a decision, you have this very narrow view of what the right decision is, and that is something that will save a life.
It doesn’t matter what else happens. You attach infinite value to stopping the disease and saving a life. You attach zero value to whether this actually totally disrupts people’s lives, ruins the economy, and has many kids kept out of school in a way that they never quite recover from.
(source)
None of this should paint public health officials as villains. Rather, it points to the need for other perspectives and voices to be included in decision-making. Science and public health can’t make value judgments, evaluate all relevant trade-offs, or fully account for human and social factors. This interview tells a story of premature consensus, excessive deference to one discipline, and the power of the resulting social pressures over discourse and social group alignment.

One last diversion before we circle back to addiction, recovery, and treatment.

This visual is intended to show the followings for the largest online shows within categories of “right-leaning” vs. “left-leaning.”
It’s easy to imagine this ecosystem growing in response to groups of people not seeing themselves reflected or respected in mainstream media, seeking alternatives, and establishing spaces for alternative experts and voices.
However, I’m less interested in the left/right categorization of these shows (many of which are disputed) than in whether they convey messages of high/low institutional trust.
Most of the red circles convey low trust or skepticism toward institutions. I’d suggest some of the blue circles also convey low levels of trust in institutions.
It’s worth noting that these low levels of trust could be related to perceptions of the integrity, effectiveness, or brokenness of institutions. The reasons for those perceptions can be wildly varying, creating loose coalitions of very strange bedfellows.
So… we have these macro-level dynamics of erosion in trust in government institutions like Medicaid and SAMHSA. As noted above, their role in funding more than half of treatment in the US means their disruption can have a massive impact on the lives of people with addictions, the people who love them, and their communities.
That’s some of what’s happening at the 20,000-foot level, but what’s happening closer to the ground?
Interestingly, 12-step recovery1 and specialty addiction treatment system2 were birthed as a response to the failures of institutions to meet the needs of people with addiction.
It’s fair to say that the field remained too skeptical of questions and information from other institutions and, as a result, was epistemically closed for far too long, maintaining orthodoxies that stifled innovation and kept the field narrow and limited in its reach and effectiveness.
As other disciplines and institutions entered the space, the result was too often a struggle for dominance rather than an effort to synthesize, integrate, and/or coordinate knowledge and methods. These struggles, however they were instigated, often intensified or resulted in more epistemic closure. As public health, mental health, and medicine moved in, old orthodoxies were replaced with new ones that reflected their worldview.
To be sure, we have our share of bad actors who challenge those orthodoxies—sometimes as 12-step one-wayers, sometimes as drug warriors, and sometimes as moralists or cultural reactionaries. Unfortunately, when good-faith actors question those orthodoxies, they get associated with ignorance or those bad-faith actors.
What are these orthodoxies?
There are several around medication, including the notion that buprenorphine can end the overdose crisis if we just get enough of it in the hands of people with opioid use disorder. There’s no question it can help reduce overdose when people take it, but there are several problems with this notion that are treated as inappropriate to note in many settings. These problems include:
- The medication’s well-documented retention problems are often overlooked in policy discussions and media reports.
- The very successful push to lower prescribing thresholds and encourage prescribing, with more than 107 million prescriptions from 2017 to 2023 without a clear impact on overdose death rates.
- States with the highest prescribing rates continue to struggle with the highest rates of overdose fatalities.
- That poly-drug problems are the norm.
When these problems are acknowledged, the solutions are to deregulate prescribing (despite more than a third of waivered doctors not prescribing buprenorphine), decriminalize street buprenorphine, and prescribe higher doses.
Other examples include:
- Decriminalization is good for public health, and the benefits are significant enough that implementation shouldn’t be contingent on the development of treatment infrastructure.
- Addiction treatment contingencies in housing first models are unnecessary, harmful, and paternalistic.
- MOUD is a complete and effective treatment and bundling them with psychosocial interventions doesn’t improve outcomes and constitutes a barrier to treatment and recovery.
- Flooding communities with naloxone is an effective prevention strategy. (Rather than one element of an effective strategy.)
- Providing a “safe supply” of drugs will be good for people with drug problems and good for public health.
- Increases in supply are not associated with increased AOD use and problems related to AOD use.
- That “recovery” should be expanded to include as many people and pathways as possible, including ongoing drug use and heavy drinking.
- That people communicating or endorsing ideas or language labeled as stigmatizing are harmful and should be delegitimized and sidelined.
- That concern about siting of low-threshold and harm reduction services is rooted in stigma and character deficiencies.
Many of these ideas were met with skepticism from the public and many stakeholders, but an environment emerged that made it difficult to ask questions or dissent in expert and advocacy spaces.
A recent addiction medicine podcast caught my attention by providing an example of a couple addiction physicians trying to deliver care rooted in evidence and best practices.
Dr. Sonya Del Tredici: I work with buprenorphine a lot, I feel like buprenorphine does a really good job of getting people off drugs, but it doesn’t magically hand you your life back. You know, to get your life back, you have to do these other elements of recovery to rebuild your relationships, your career, your finances, your health… that’s a process.
Dr. John Keenan: I feel like there’s a pendulum swinging here. When I started, I think we had kind of more of an abstinence-only approach. Everyone kind of participated with an abstinence-only program here and in our community, and then I feel like we’ve swung to now this kind of risk-reduction… just medication at the office visit kind of approach, and I feel like I found myself swinging back, hopefully somewhere to the middle. I feel like different people need different things, but if you’re not incorporating these elements into your life, or at least you don’t even value them… I guess that’s the first thing… like what do you value? I just feel like, eventually, we’re going to have a problem at some point. Not between me and the person, but I feel like there’s going to be some sort of thing that rocks the boat and it’s going to lead to an outcome that the person doesn’t want.
Dr. Sonya Del Tredici: Agreed. Your recovery is more vulnerable if you don’t have these other tools. Also, I see some people who are kind of stuck… they’ve gotten off drugs, but they haven’t they haven’t really achieved other life goals, and I want to help them achieve all their goals.
What is Recovery? on the Addiction Medicine Journal Club podcast
These providers suffered from a professional environment that lacked voices asking questions about the differences between recovery and stabilization or remission. Many people with lived experience could have pointed to these gaps in their care model. I’ve no doubt that recovery peer support specialists could have provided valuable information about these gaps, but the treatment and professional environment haven’t welcomed those discussions.
None of this is to say that the system should be dismantled or destroyed. I’m genuinely afraid for people with addiction, their families, their communities, and for addiction professionals. However, like a lot of other institutions/systems/spaces, the system has needed disruption and has deployed something like an immune response to resist disruption.
I see a lot of parallels—premature policy consensus, an unwillingness to re-examine assumptions, and intolerance of criticism and divergent points of view—all of which hurt our policy responses and our ability to course correct as we learned more and had greater reason to course correct.
All that relates to the symbolic capitalists3 (AKA elites, the Professional Managerial Class, the New Class, the Creative Class, etc.) in the space. Combine this with the treatment and recovery hustlers and entrepreneurs who exploit despair and provide an example of bad faith that helps perpetuate the cycles described above.
None of this is unique to our space or this moment. Current orthodoxies emerged to replace old orthodoxies, and treatment systems have collapsed in earlier eras. In 1999, Bill White imagined what a future existential threat might look like.
If the field of addiction treatment should face extinction again, it will likely not be from one but a combination of contextual and internal threats. The worst potential scenario would be a sudden and sustained downturn in the economy and a concurrent increase in social disorder. Such a combination would have public and private policy leaders making tough choices regarding the allocation of resources and doing so within a climate of fear that could shift the focus from one of treating addicts to one of sequestering and punishing addicts. The most likely scenario would be the destruction of addiction treatment as a categorically segregated enterprise, the widespread integration (merger) of addiction treatment into more powerful health and human service entities, and the illusion of continued service availability while large numbers of alcoholics and addicts are moved from the public health arena to the criminal justice arena. This scenario could happen only in the face of a weakened field of addiction treatment, vulnerable in the marketplace of ideas about who should have cultural ownership of this problem, vulnerable in terms of the field’s scientific and public credibility, vulnerable from the loss of the grassroots movement that birthed and sustained it, and vulnerable from the lack of statespeople to lead a response to such threats.
To prevent such a scenario, we must rebirth the grass roots movement that laid the cultural foundation for the rise of 20th century addiction medicine and the modern system of addiction treatment. We must both aggressively monitor the ecosystem within which we operate and take a more activist role within that ecosystem. We must get ourselves clinically and ethically recentered. We must take a highly splintered field and find a way to speak with one voice. And we must rebirth a new generation of leaders who can carry our mission of serving the still suffering addict into the 21st century. If we fail to meet these challenges, we may be doomed to repeat an episode in history little known to today’s providers of addiction treatment. And that lack of knowledge is perhaps itself a source of great vulnerability. As the great comedic scholar Lilly Tomlin once suggested, “Maybe if we listened, history wouldn’t keep repeating itself.”
White, W. (1999). Addiction treatment: Gone yesterday, gone tomorrow? Behavioral Health Management, 19(5), 40-44.
What would cutting access to care mean for the field, people with addiction, their families, our communities, and addiction counseling? It’s hard to know exactly, but we know that addiction won’t disappear. We’ve known the effects of untreated addiction — mortality will increase, crime will increase, incarceration will increase, demands on the child welfare systems will increase, health care costs will increase, need for social services will increase, homelessness will increase, and employers will deal with increases in AOD related problems with few resources to help employees. Most importantly, people will addictions will suffer more and longer. Their children, their parents, everyone who loves them will suffer too.
We don’t have all the answers. Treatment often doesn’t result in recovery, or it takes multiple attempts to achieve stable recovery. We also know treatment has been a pathway to recovery from addiction and has improved the lives of millions of people in small, large, and transformational ways. Disruption, not destruction, is needed and I hope that people can make the changes needed to drive constructive disruption.
- From William White in Slaying the Dragon (2014): “During the early 1930s, the woes of America’s alcoholics were increasing, just as earlier sources of help for the alcoholic had all but vanished. By 1930, most of the early-20th-century “drying-out” institutions had closed their doors, and those that remained were closed to all but the most affluent or well-connected alcoholics. Overcrowded city hospitals and state psychiatric hospitals discouraged admission of alcoholics, and aggressively advertised home cures for alcoholism were rife with fraud. A.A. was born amidst the inability of more formal helping institutions to respond successfully to the problem of alcoholism.
Alcoholics entered the mid-1930s in need of help, but highly skeptical. Their families–whose suffering had also intensified amidst the drying-up of public and private charities–were at their wits’ end, but equally skeptical that anything could help. A vacuum of need existed that begged to be filled with a source of hope.” ↩︎ - From William White in A history of contempt (2003): “The field of addiction treatment emerged as a segregated field of professional service in the 1970s because the lay and professional leaders of that field were convinced by their study of history and their own collective experiences that alcoholics and addicts would not be welcomed nor would they ever get the care they needed within mainstream mental health, public health, and social service agencies. The majority of those who birthed this specialty field knew from their own personal experience just how inept mainstream institutions were at treating the alcoholic/addict and that the best interests of alcoholics/addicts were unlikely to be served in such institutions. They also knew that this was a failure both of technology (misguided assumptions and ineffective methods of intervention) and of attitudes. Those understandings became the impetus for a re-birthed field of addiction treatment and new specialty roles in addiction medicine and addiction counseling.” ↩︎
- See Language, social justice, access to care, symbolic capital, and recovery advocacy: Symbolic capitalists (AKA the Professional Managerial Class, the New Class, the Creative Class, etc.) who “make a living primarily based on what they know, who they know, and how they’re known. Symbolic capitalists are professionals who traffic in symbols and rhetoric, images and narratives, data and analysis, ideas and abstraction (as opposed to workers engaged in manual forms of labor tied to physical goods and services).” “Their work involves the production and manipulation of information, rhetoric, social perceptions and relations, organizational structures and relations, traditions and innovations, and so on. Those who work in fields like education, science and technology, finance and accounting, arts and entertainment, media, law, consulting, administration or public policy are typically symbolic capitalists.” (source) ↩︎

Depressing to witness this again in my lifetime. But the current regime is destroying the entire system of governance in our country and, much as we like to self reflect over our own shortcomings, sometimes we are just victims of the times and have to repeat the mistakes of the past. We went through this with Department of Corrections. This too shall pass but, the people we serve along with their families and the communities will suffer because of this shortsightedness.
LikeLike