
A recent letter to JAMA analyzes the National Survey of Drug Use and Health regarding the need for treatment:
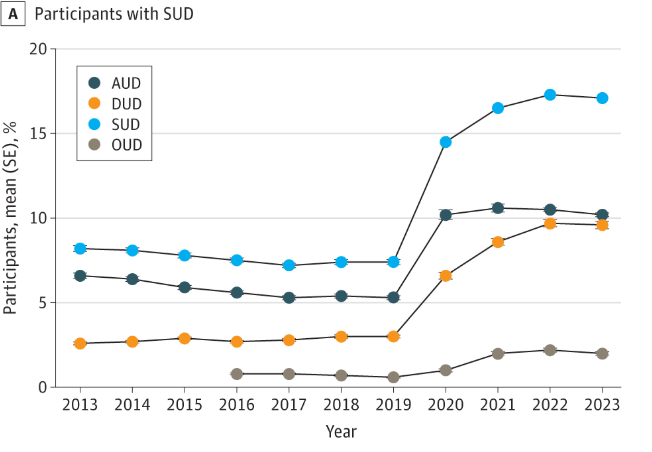
Among 657 583 participants, the prevalence of individuals needing SUD treatment increased from 8.2% in 2013 to 17.1% in 2023. AUD increased from 6.6% to 10.2%, while DUD increased from 2.6% to 9.6%. OUD more than doubled from 0.8% in 2016 to 2.0% in 2023.
Liu L, Zhang C, Nahata MC. Trends in Treatment Need and Receipt for Substance Use Disorders in the US. JAMA Netw Open. 2025;8(1):e2453317. doi:10.1001/jamanetworkopen.2024.53317
So… in a period of 10 years, the need for SUD treatment increased by 108.5%? The need for AUD treatment increased by 54.5%? The need for OUD treatment increased by 150%? More than 1 in 6 Americans need SUD treatment in the past year?
What should we make of this?
As discussed in a previous post (below) this likely has a lot to do with DSM5 criteria being too inclusive.
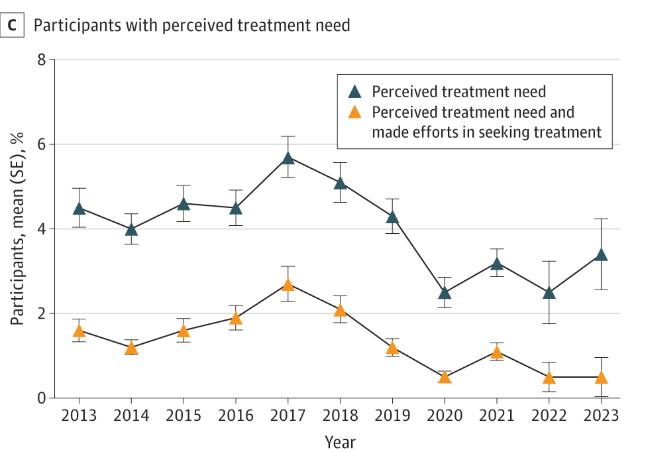
The letter also notes declines in people with SUDs perceiving a need for treatment and receiving treatment. This should not be a surprise when the denominators have exploded.
Several years ago, Jerome Wakefield wrote a response speaking to this issue in the transition from the DSM IV to the DSM 5:
‘Abuse’ has long been a questionable disorder category.
…To its credit, DSM-5 finally eliminated the substance abuse category. However, rather than acknowledging that the abuse category lacks conceptual validity as an addictive disorder and placing it in the Z Codes for non-disordered problems often treated by clinicians, DSM-5 took another route. Much of the abuse category was assimilated to dependence, in keeping with the empirically discredited ‘mild or prodromal dependence’ account of abuse.
…With so many more symptom options in SUD than in the former dependence category, it becomes much easier for an individual to meet three criteria. Thus, one might think that to maintain validity, the threshold number of symptoms needed for diagnosis would be raised to a higher number. This would be especially true because the added abuse symptoms appear to have less validity than the former dependence symptoms in identifying impaired-control dysfunction. Thus, the number of symptoms needed to have confidence that there is a dysfunction should be increased.
The workgroup did the opposite; they lowered the number of symptoms required for diagnosis to 2. This is probably the most controversial substance-related change made by the DSM-5. If one considers SUD an expanded impaired-control addiction category analogous to dependence, then this change dramatically increases—indeed, more than doubles—the estimated prevalence of addiction.
Wakefield, J.C. (2015), DSM-5 substance use disorder: how conceptual missteps weakened the foundations of the addictive disorders field. Acta Psychiatr Scand, 132: 327-334. https://doi.org/10.1111/acps.12446
So, it’s not at all surprising that the percentage of people perceiving a need for treatment declined and the percentage of people receiving treatment declined when this public health data is rooted in questionable criteria making the diagnosis questionable for millions of people.
This speaks to the importance of the right criteria, the right diagnosis, the right response, and the right conceptual framework. This is a good example of how bad conceptual boundaries can have unintended downstream effects, become self-reinforcing, and drive policy in unanticipated directions.
A previous post on the NSDUH and this category problem is below.
Substance use disorder is too inclusive to be useful
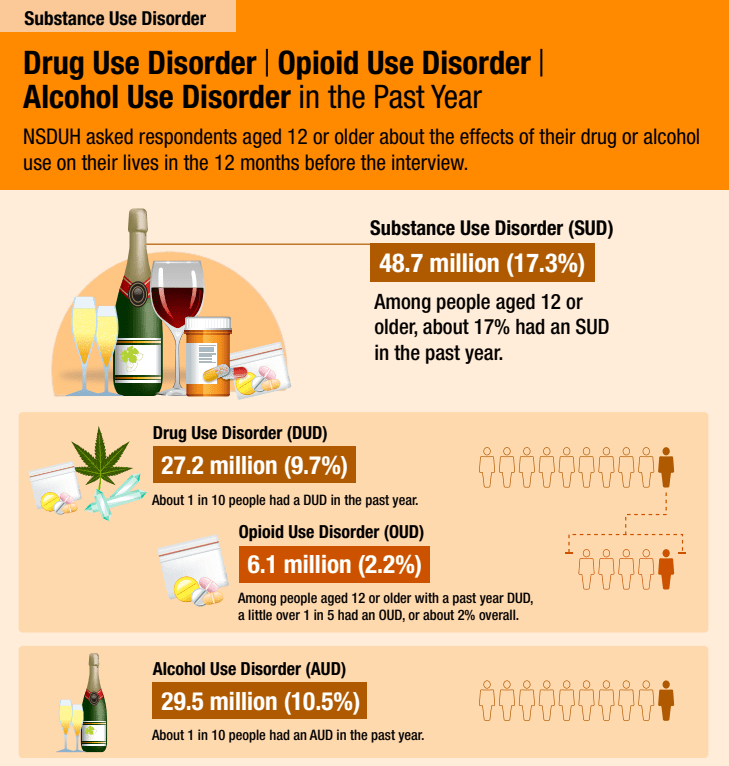
The 2022 National Survey on Drug Use and Health was recently released and it reports, using DSM-5 criteria, that 17.3% of Americans 12 or older (48.7 million people) had a substance use disorder (SUD) in the past year.
For context, the 2020 National Survey on Drug Use and Health, the first year using DSM-5 criteria, reported that 14.5% of Americans 12 or older had a substance use disorder (SUD) in the past year.
And, according to the 2012 National Survey on Drug Use and Health, using DSM-IV criteria, 8.5% of Americans 12 or older met criteria for past-year Alcohol or Drug Dependence or Abuse.
At what point do we recognize that the term substance use disorder doesn’t tell us much? It’s too inclusive to mean much of anything.
How high will it go? If more than one in six Americans 12 or older have a past year SUD, what’s the lifetime prevalence?
As a category, SUD is about as helpful as pulmonary disease. It tells you something about the likely symptoms, but it could be acute, it could be chronic, it could be mild, it could be severe, it could be a minor inconvenience, or it could be disabling and something that shapes the person’s identity.
It tells us nothing about the nature of the problem, the cause, the course, the severity, whether it requires treatment, the kind of treatment indicated, what problem resolution (recovery) looks like, or the implications for the patient, their loved ones, and the community.
Of course, this isn’t news and it’s not without consequence.
But, there is a way to differentiate chronic and severe problems from other types of SUDs.
One more thought: Maybe SUD is useful at the population level. If that’s true, what are the consequences of a diagnostic category that is much more useful at a population level and not particularly useful for treatment? What pressures does that create for treatment systems? What blindspots does it create for systems of care?

2 thoughts on “Substance use disorder sets off a cascade of category errors”
Comments are closed.