
“Multiple pathways to recovery” has been popularized by the new recovery advocacy movement (NRAM) and Recovery Oriented Systems of Care (ROSC), but the concept has been around since at least 1944.
The September 1944 issue of Alcoholics Anonymous’ Grapevine published an article by Philip Wylie, describing his solo recovery supported by psychologists and reading.
Bill Wilson wrote an accompanying column and included the following statement: “…no AA should be disturbed if he cannot fully agree with all of Mr. Wylie’s truly stimulating discourse. Rather shall we reflect that the roads to recovery are many; that any story or theory of recovery from one who has trod the highway is bound to contain much truth.”
Despite Wilson’s explicit validation, it didn’t catch on. “Recovery” identities were generally only claimed by people in 12-step recovery. Accordingly, the larger culture generally associated the word with 12-step recovery.
This invites questions about what we mean by “pathways to recovery.”
A pathway leads from one place to another, so there are 3 elements: 1) the starting point (the condition people are recovering from); 2) the pathway; and 3) the destination (or endpoint, in clinical spaces).
Before the New Recovery Advocacy Movement
Let’s look at the pre-NRAM popular understanding of recovery.

The starting point had been confined to alcohol and other drug (AOD) addiction, the most severe form of AOD problems. (Though it is worth noting that addiction treatment providers had a false-positive problem, particularly among adolescents and young adults.)
The pathway had generally been confined to 12 step programs, though faith communities may have created space for recovery through a religious conversion pathway.
The destination within this model was unambiguously abstinence. AA’s text says “The only relief we have to suggest is entire abstinence.” NA’s text says “This is a program of complete abstinence from all drugs.“
It’s worth noting that AA framed the problem as alcohol and, officially, “abstinence” refers to alcohol only. The boundaries of “abstinence” varies from group to group and member to member. NA made an interesting change the first step. Rather than changing “alcohol” to “drugs”, they framed the problem as “addiction”, framing their drug use a symptom of an illness–addiction.
However, both AA and NA make it clear that abstinence is necessary but not sufficient. AA’s text says, “We feel a man is unthinking when he says that sobriety is enough.” NA’s text says, “Our disease involves much more than using, and so our recovery must involve much more than simple abstinence. Recovery is an active change of our ideas and attitudes.”
Both programs characterize recovery as requiring abstinence plus a change in behaviors and attitudes. (Which makes it simultaneously a process and an outcome.) Some people have used this as the foundation for describing “better than well” recovery where the person with the addiction achieves much more than remission. The experience of recovering from a seemingly hopeless condition through a new way of life and fellowship might be framed as something akin to post-traumatic growth. (For the rest of the post, I’ll refer to this as abstinence+.)
Too Narrow
The emergence of the New Recovery Advocacy Movement and Recovery-Oriented Systems of Care brought attention to the narrowness of this model of recovery. Specifically, there were concerns that it excluded methadone patients (buprenorphine was not yet FDA approved) and that it excluded non-12-step mutual aid.
This is when we began hearing more about “multiple pathways to recovery” and the need for recognition, validation, and celebration of other pathways to recovery.

It’s important to note two things about this:
- First, there was no change to the starting point or the destination. (In fact, the message that recovery is more than abstinence was used to raise the bar for treatment providers.)
- Second, this message of multiple pathways was a call for change at the levels of research, treatment, advocacy, and community.
Advocacy Changes Boundaries
A key message of the NRAM was that addiction had been very visible and recovery had been invisible. It was believed to be important to make recovery visible to reduce stigma and kindle hope for recovery from addiction. One of the messages was that recovery is much more prevalent than the public realized. A key point to support this message was that spontaneous (or natural) recovery was common.
An important caveat often left out, was that these cases of spontaneous recovery frequently occur in less complex, less severe, and less chronic AOD problems.
This slipped in a couple of important changes. The inclusion of spontaneous recoveries didn’t just add a pathway but also introduced changes in the starting point and the destination.
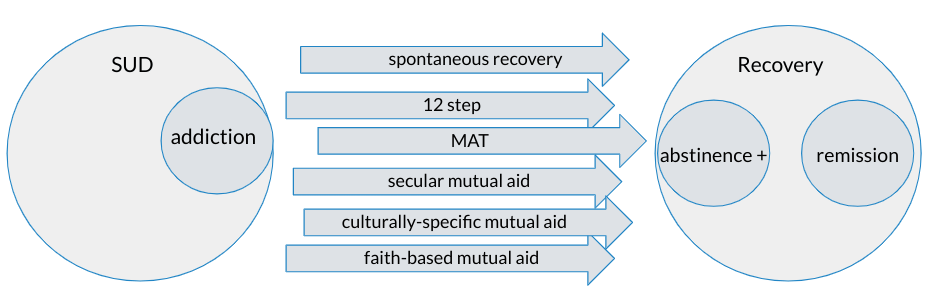
These cases expanded the starting point from people with addiction to people will less severe and chronic AOD problems.
These cases also expanded the destination from traditional notions of recovery being abstinence+ to include remission.
This community advocacy message was not perfectly aligned with advocacy in clinical contexts to distinguish recovery from remission.
Remission is about the subtraction of pathology; recovery is ultimately about the achievement of global (physical, emotional, relational, spiritual) health, social functioning, and quality of life in the community.
White, W. & Torres, L. (2010). Recovery-oriented methadone maintenance. Chicago, IL: Great Lakes Addiction Technology Transfer Center, Philadelphia Department of Behavioral Health and Mental Retardation Services and Northeast Addiction Technology Transfer Center
Another important change was that the addition of these “spontaneous recoveries” and “remission” meant the addition of people who achieved remission through moderation and have never considered themselves to be in recovery or adopted a recovery identity.
Explosions in the prevalence of substance problems and recovery
How many people are in recovery?

All of this sparked interest in better understanding the actual prevalence of recovery, which inspired research on that question.
In the years since, several studies have been done and estimates of Americans in “recovery” ranged from 20,000,000 to 23,000,000 (or 9-10% of all adults).
That’s a stunning number. BUT, it’s important to consider how researchers arrived at those numbers. Most of these studies are based on surveys asking whether respondents “used to have a problem with drugs or alcohol but no longer do.”
Anyone who answered that question was categorized as in recovery, even though most of those respondents do not consider themselves to be in recovery.
How many people have addiction?

The 2022 National Survey on Drug Use and Health was recently released and it reports, using DSM-5 criteria, that 17.3% of Americans 12 or older (48.7 million people) had a substance use disorder (SUD) in the past year.
For context, the 2020 National Survey on Drug Use and Health, the first year using DSM-5 criteria, reported that 14.5% of Americans 12 or older had a substance use disorder (SUD) in the past year.
And, according to the 2012 National Survey on Drug Use and Health, using DSM-IV criteria, 8.5% of Americans 12 or older met criteria for past-year Alcohol or Drug Dependence or Abuse.
It’s important to note that these are not reports of lifetime prevalence, they are reports of past year prevalence. Lifetime prevalence would be much higher.
This is a problem because addiction and SUD are routinely conflated, not just at the public level, but also in the media and academic publications. A big contributor to this is the lack of clear definitional boundaries for addiction, but there is a way to differentiate chronic and severe problems from other types of SUDs.
Recovery Messaging
One tactic deployed by the NRAM to combat stigma and raise awareness of recovery was recovery messaging training. This messaging education emphasized that recovery meant no longer using AOD, that it was stable (“long-term”), and that it involved more than abstinence (abstinence+).

A short time later, most visible in the film The Anonymous People, we started to see a shift from “I’m in recovery, what that means…” to “I’m in recovery and, for me, that means…”
Also, around this time, CCAR, the most prominent and influential Recovery Community Organization (RCO) too the position that participants are “in recovery if you say you are.”
This was not meant as a statement about the definition of the conceptual boundaries of recovery. Rather, it was an organizational stance about how they would engage and work with participants — that they are not going to gatekeep or argue with any participant who identifies as recovering. It was a statement that their approach will be to engage participants in discussions about what recovery means to them, why they believe they are in recovery, and how their approach is (or is not) working for them.
This organizational stance became an organizing slogan for much of the NRAM.
These changes in the way recovery is represented represent a profound shift in how recovery’s boundaries are drawn — from boundaries drawn by groups and communities of recovery to boundaries being drawn by individuals, meaning there are nearly infinite pathways and definitions of recovery (destinations).
Other disruptions in pathways and conceptual boundaries
- The Chicago Recovery Alliance defining recovery as “any positive change” and the popularization of this definition by the book Undoing Drugs.
- This leads to the growth of the belief that harm reduction isn’t just a pathway to recovery, but that it is recovery in-and-of-itself.
- It also expands the starting point to people who use drugs (PWUD) rather than limiting it to people identified as having an AOD problem.
- The dissemination of new recovery definitions
- “Recovery from substance dependence is a voluntarily maintained lifestyle characterized by sobriety, personal health, and citizenship.” (Betty Ford Consensus Panel, 2007)
- “A process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential.” (SAMHSA, 2010)
- “Recovery is a process through which an individual pursues both remission from alcohol use disorder (AUD) and cessation from heavy drinking. An individual may be considered “recovered” if both remission from AUD and cessation from heavy drinking are achieved and maintained over time.” (NIAAA, 2017)
- Recovery research leaders deconstructing addiction and recovery
- Efforts to “depathologize addiction”
- Asserting that “recovery” is loaded with concepts that stigmatize
- Describes “clients rejecting recovery label” (this invites questions about who is labeling them)
- Asserts that recovery can include heavy drinking
- Asserts that abstinence is stigmatizing
- The growth of substance-specific recovery (recovery from opioid use disorder, alcohol use disorder, etc.)
- The emergence of concepts like plant-based recovery that involve ongoing use of substances like kratom, cannabis, and psychedelics.
Process, direction, outcome?
Long before researchers and scholars took an interest in recovery, recovering people have described recovery as a process. What’s interesting here, is that I think recovering people have thought of recovery as a process and a destination/outcome. Some might think of it as a process that leads to an outcome, while others might think of it as an outcome maintained by a process. Whatever the case, both elements are considered essential. The Betty Ford Consensus Panel definition integrates a lifestyle (destination) that is voluntarily maintained (process). This more recent wave of definitions emphasizes a process and a direction (“improvement . . . striving . . . full potential” and “sustained efforts to improve wellness”) rather than an outcome or destination.
Recovery Today
Advocacy to advance multiple pathways has resulted in the recognition of many new pathways. It has also resulted in dramatic changes to the starting point and destination.

The purpose of this post isn’t to lament change. Different people will have different perspectives of what’s good or not-so-good.
My goal is to help make visible the water we’re swimming in, so we can think through the implications of all this.
- Which destinations are appropriate for which starting points?
- Is someone using a “pathway” if they are developing a pathway that works for them? (as opposed to trailblazing?)
- What disagreements are likely to arise due people having different conceptions of the problem, the pathways, and the meaning of recovery?
- Where might this work well and where might it be unhelpful? For example, even if we believe the original meaning of recovery was too narrow, are current understandings useful for systems and practitioners as a clinical endpoint?
- When defining the boundaries for something like recovery, what characteristics are useful in different spaces like advocacy, research, treatment, peer work, family work, community education, and system design?
- Was recovery the right construct to try and build a system around? Or, would we have been better off with something more like Brian’s stages of healing?

Well written.
LikeLike