
Between 1919 and 1923, clinics provided legal access to narcotics to treat addiction
In 1923, Oscar Dowling brought a serious charge against a doctor in Shreveport, Louisiana. Like a headline we’d recognize today, he claimed the doctor prescribed, “indiscriminately … of morphine in excess,” and had turned the wealthy Shreveport into a mecca for junkies and drifters. But this was no corrupt doc. In fact, the local medical community came to his defense – because of the doctor’s effort, they claimed, Shreveport had rid itself of drug trafficking.1 And it resulted from his radical new way of addressing addiction: dispensing legal morphine through “narcotic clinics.”
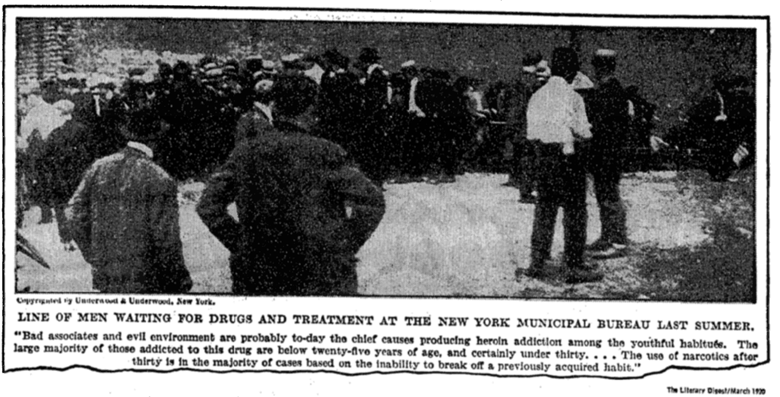
Shreveport, Louisiana was home to just one of 44 narcotic clinics2 that once existed across the country. For a few short years, opiate dependent men and women lined up at doors in New Haven, Los Angeles, Jacksonville, New York City,2–4 and were dispensed a daily dose of morphine (sometimes heroin or cocaine), under medical supervision.
It’s a forgotten chapter in the history of addiction treatment, but one that tells a very different story of how communities once thought about the problem of addiction. Each clinic offered a humane alternative to federal policy that was aggressively criminalizing addiction, 12 years before AA, and over 40 years before the introduction of methadone maintenance.
What Caused the Clinics to Open?
“Our present mode of [pain] treatment offers little that is satisfactory,” physician Alexander Wood opened in an 1855 pamphlet, but in its pages he described a new “method of treatment…generally palliative, and often curative”. By the mid-19th century, medicine seemed to have cured pain; the delivery of morphine through the hypodermic syringe, invented by Wood, could provide relief in cases where medicine was once powerless. The effect was almost mystical: “In ten minutes it takes one out of a world of pain, and transfers him to a world of unspeakable content…’words is vain to expredge it.’” (Dr. Henry Gibbons of San Francisco, 1870).
By 1881, almost every American physician used the instrument, and with the profession hypnotized by its new found power, morphine became a solution for almost every ailment (even, “masturbation, photophobia, [and] nymphomania”). By the end of the 19th century, approximately 1 in every 200 Americans was addicted, most introduced by prescription.5
The medical profession corrected itself in due time. Recommendations for lighter opiate use were spread and prescriptions decreased. But a cultural panic about addiction subsisted, made worse by America’s real fears: immigration, poverty, and racial integration. Where the 19th century addict was introduced to drugs through medicine, Americans in the early 20th century began to stereotype minorities as addicts and their drug use as the source of urban street crime.
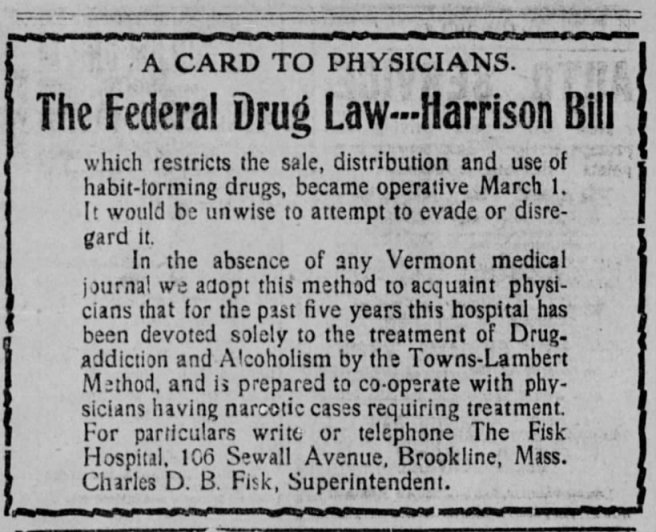
States, and then the federal government, passed legislation criminalizing drug use (notably the Harrison Narcotics Tax Act), and banned the ability for physicians to prescribe narcotics for the purpose of addiction maintenance (i.e., to stave off withdrawal). The fact this was a target of policy suggests it was common enough, and, in fact, about 25,000 physicians were convicted by the Act between 1914 and 1938.6 Supreme court rulings in 1919 held these convictions were constitutional, turning doctors into criminals and sending communities searching for solutions.
The Opening and Running of the Clinics
Dr. W. M. Swords knew little about addiction. But he became an unwitting participant in its treatment. Swords was one of many physicians visited by concerned public officials and desperate people with addiction following the 1919 decisions, who searched for a solution now that maintenance was closed off. People who could formerly maintain their use with decency visited Swords, a New Orleans physician, and pleaded with him to reopen the valve. In mercy, he allowed daily doses of morphine for three people in February of 1919. Within two weeks, Dr. Swords was being visited by between 300 and 500 people on a daily basis, and his experiment grew into Louisiana’s first narcotic clinic.7
Concern for safety and suffering drove clinics to open up in 1919. The move to criminalize physician maintenance was celebrated by federal enforcement, but the impact was more complicated at a local level. Communities recognized that suddenly cutting off their citizens would only lead to more crime and trafficking. In lieu of federal support, more than 40 local clinics opened around 1919, many led by city health officials, local physicians, and law enforcement.8
Conditions varied from clinic to clinic. Some were well-run and some only reflected the bleakness of addiction. In New York City, the clinic operated in such crowded conditions that lines snaked “a block or more” down the street in any weather. Dosages were described as “arbitrary”, often far more than what was needed, and then just as arbitrarily tapered until patients were sent back to the streets. Handling over 500 patients a day made clinic operations unorganized and confusing; some cycled through the line repeatedly to get extra doses. The clinic survived only nine months.3,8

Shreveport, on the other hand, was the model narcotic clinic. Encouraged by the New Orleans experiment, board of health president Oscar Dowling approached physician Willis P. Butler to launch a similar program in Shreveport. Dr. Butler put his focus on “incurables”, people with long addiction histories and inoperable medical conditions who were unlikely to respond to treatment. The Shreveport clinic operated within a hospital, and was supported by an adjacent detox facility, a venereal disease clinic, and nursing staff. The “incurables” were maintained on a stable dose of morphine; younger and healthier patients were directed to detox. Local newspapers praised the program and credited it with a sharp reduction in drug-related crime in 1920; it diverted potential criminals into stable, productive lives.1,9
What Caused the Clinics to Close?
The narcotic clinics were doomed from their start. After 1919, there was virtually no federal support for the programs.8 Some in the Treasury Department (formerly responsible for drug enforcement) had, for a short while, entertained support for the clinics. As the Treasury’s commissioner of internal review wrote in response to the Supreme Court decisions, a “system of relief” was needed, “whereby these unfortunate persons may be prevented from becoming menaces to the community,” and offered that narcotic clinics could be that relief by providing users “the minimum dose required to prevent their physical and nervous collapse.”
But your average Treasury official saw addiction as a criminal problem. 1919 was a year of great federal moralizing; it was the passing of the National Prohibition Act which, besides banning alcohol, put Prohibition agents in charge of narcotic enforcement. Prohibition agents saw addiction as a supply side issue: eliminate as many drugs and alcohol as possible and the problem will go away.8 Narcotics clinics were part of the supply, and their existence was a threat to America’s emerging preference for criminalization.
Internally, the Treasury Department decided to close the clinics in winter of 1919-1920.8 They only needed a public reason to quell opposition. They had their evidence with the failure of the New York Clinic. Well into the 1960s, drug enforcement agencies would cite the New York Clinic as proof of the absolute failure of the narcotics clinics. While they were correct that fraud pervaded the program, they would also make dubious claims that the clinic was in the business of “making new addicts”, apparently by exposing innocent family members to the temptations of drugs as they were enlisted to procure extra doses for relatives.
There’s great power to horror stories, and reports from New York’s clinic gave the Treasury what it needed to threaten physicians with arrest. Treasury officials thought they might face a fight with medical community, but the threat alone caused most clinics to close “voluntarily” between 1919 and 1921.
Shreveport, however, was a stubborn holdout. In the sort of spectacular ineptitude that only federal agencies can display, the Treasury sent agents on multiple occasions to either catch Willis Butler breaking the law or at least buy narcotics on the streets of Shreveport, both of which were unsuccessful. Dr. Butler would describe one sorry agent the Treasury sent who was himself addicted, forcing Butler to confront him for stealing the morphine he was meant to be inspecting.9
The betrayal by Oscar Dowling, however, was harder for Butler to shake. Dowling, a friend, had enlisted Butler to start the clinic in 1919, but a few years later was attempting to have him arrested. Behind the scenes, Dowling was facing heavy pressure from the Treasury Department to crack down on clinics in his state. While the case went his way, Dr. Butler foresaw an endless battle with federal authorities, and he closed the last narcotic clinic in 1923.1
The Clinics’ Legacy
“Since 1923, there has been no attempt to revive any public facility for the treatment of addicts on an out-patient basis,” attorney Rufus King would write in 1957, discussing the legacy of the clinics. It was written almost a decade before the first methadone maintenance clinic would open in New York City. The Fed’s crackdown set back addiction medicine by decades: “[Physicians] were driven into full retreat by a series of Supreme Court decisions…” wrote King, “any prescribing for an addict…was likely to mean trouble with the Treasury agents.”
Bill White would say that closing the clinic drove “the final wedge between physicians and their addict patients.”3 And perhaps that wound hasn’t healed. In over 200 studies in the last 61 years that asked doctors why they feel reluctant to treat addiction, the most commonly cited reasons were “institutional barriers”: a lack of leadership support for addiction intervention, lack of training, and, echoing the clinics, concerns about red tape and legal liability. Compassionate physicians like Willis Butler still exist, but the system remains haunted by the specter of drug enforcement.
References
1. Waldorf D, Others A. Morphine Maintenance: The Shreveport Clinic 1919-1923. Special Studies No. 1. Publications, Drug Abuse Council, Inc; 1974. Accessed December 4, 2025. https://eric.ed.gov/?id=ED109516
2. Kolb L, Mez AGD. The Prevalence and Trend of Drug Addiction in the United States and Factors Influencing It. Public Health Reports (1896-1970). 1924;39(21):1179-1204. doi:10.2307/4577168
3. White W.L. Slaying the Dragon: The History of Addiction Treatment and Recovery in America. Chestnut Health Systems; 2014.
4. Baumohl J. Maintaining Orthodoxy: The Depression-Era Struggle over Morphine Maintenance in California. Contemporary Drug Problems. 2000;27(1):17-75. doi:10.1177/009145090002700103
5. Courtwright DT. Dark Paradise: A History of Opiate Addiction in America. Harvard University Press; 2009.
6. Eriator I. Opioid Use in the United States. Federal Practioner. Published online 2003. Accessed December 4, 2025. https://cdn.mdedge.com/files/s3fs-public/Document/September-2017/020110050.pdf
7. Tallaksen A. The narcotic clinic in New Orleans, 1919-21. Addiction. 2017;112(9):1680-1685. doi:10.1111/add.13867
8. Musto DF. The American Disease: Origins of Narcotic Control. Oxford University Press; 1999.
9. Courtwright DT, Joseph H, Jarlais DD. Addicts Who Survived: An Oral History of Narcotic Use in America before 1965. University of Tennessee Press; 1989.
