
Here, the 5 year model monograph is reduced to a one-pager. The notion of reducing the monograph to a one-pager was given to me by Katlyn Nordstrom, and I greatly appreciate that suggestion.
What follows is the content of the one-pager. I’m guessing I might continue to adapt the material in the monograph into tools closer to ready for real-world practical application by working clinicians.
5 years of clinical engagement for one person with a complex, chronic and severe SUD are shown below.
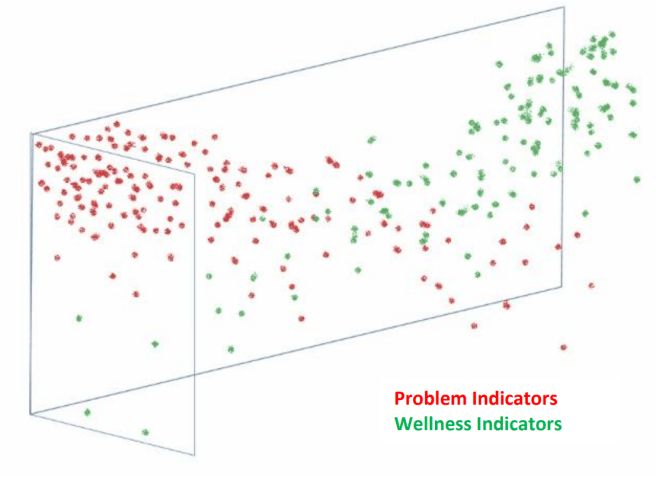
“5 years” is the answer to the question: “When does present sobriety/remission predict lifetime sobriety/remission?” The starting point for the clinician is the universal benchmark of sustained remission and improving quality of life five years after the last clinical touch. As shown, during the five years of care, the active problem indicators are becoming fewer and are falling. And the active wellness indicators are increasing in number and are rising. At the start some wellness indicators are present. And at five years some problem indicators are still present.
Critical thresholds are as follows:
- First 4 appointments. If the patient makes the fourth appointment, the intake or transfer was a “take”. Until they come to their fourth appointment, one does not know.
- 30th day. Drop out is highest in the first 30 days.
- 90 days. After this point relapse risk levels off; SUD early remission.
- 1 year. After this point relapse risk levels off; SUD sustained remission.
- 2 years. At this point improvements from year 1 are maintained; relapse risk levels off.
- 5 years. If the patient gets to year five their risk of relapse returns to the base rate of occurrence of the general population and they are in remission as with other chronic diseases.
System form and function:
- The psychology of chronic illness is the milieu within which the clinical targets reside.
- Do not assume associated clinical problems are less important than the SUD itself.
- Apply the universal benchmarks of wellbeing.
- All clinical methods should be available.
- Group therapy, Individual counseling, Coaching, Check-ups: sustained and individualized.
- Outcomes are rolled back in for individualization of care.
A significant number of clinical targets are pre-identified from the relevant experimental and clinical literature. Some are brought in by the individual patient’s case data. Some clinical targets represent milestones of improvement, some are only relevant within specific critical thresholds of time, and some targets remain relevant throughout the duration of service.
Focus Areas of the Patient-Clinician Team (to be read as columns)
| Patient Activities | Clinician Activities | Shared Responsibility |
| The six core processes: | Routine check-up intervals. Group and individual counseling. Adjust dose, frequency, and duration. | Process management: |
| Self-efficacy (in-gear effort, as pursuit, in the “do” direction) | Provide clinical service with predetermined stage-specific relevance. Data concerning the patient’s condition is recursive to care. Clinical service and check-up schedules are adjusted in emerging responses to new information. | Development of: emotion experiencing, mindfulness, acceptance, sense of self, meta-cognition, the relationship, attentional flexibility, values, cognitive flexibility, defusion/distancing. |
| Distress tolerance (mindfulness-clutch, as release) | Assist in development of: emotion experiencing, mindfulness, acceptance, sense of self, meta-cognition, the relationship, attentional flexibility, values, cognitive flexibility, defusion/distancing. | Development of: 1) Self‐awareness; 2) Empathy; 3) Mentalizing |
| Self-inventory | Assist in development of: 1) Self‐awareness; 2) Empathy; 3) Mentalizing | Illness self-management process |
| Telling on one’s illness | As critical thresholds of time and progress are met, move on to the targets and methods specific to the next relevant window of time | 2. Monitor & manage 3 areas: 1) Problem indicators 2) Wellness indicators 3) Core processes |
| Apply disease management knowledge and skills | Provide a Balint group method through years 3-5 focused on recovery management. | |
| Apply recovery management knowledge and skills |
Reference: Coon, B. April 8, 2025. 5 Year Continuing Care System for High Severity, Complexity, and Chronicity SUD’s: Clinical Targets, Methods, and Increments of Time. (2022 monograph). RM/ROSC Library of the William White archives: Chestnut.
Here’s a PDF of the one-pager for those that would find it helpful to have one.
