
I’m sharing this to supplement yesterday’s post on retiring the concept of deaths of despair. A version of this post was originally published in 2018 and is part of an ongoing review of past posts about the conceptual boundaries of addiction, the disease model, and recovery.

The narrative that the opioid and overdose crisis is a product of despair has become very popular. The logic is that people in bad economic conditions are more likely to turn to opioids to cope with their circumstances and that their hopeless environmental conditions make them more likely to die of an overdose. This model frames addiction and overdose as diseases of despair.
This model fits nicely with other writers who have garnered a lot of attention on the internet.
- Johann Hari presents addiction as a product of a lack of connection to others.
- Carl Hart frames sociological factors as causative and argues that there’s a rationality to escaping terrible circumstances via drug use and that a form of learned helplessness eventually takes root.
- Bruce Alexander is frequently cited to support these theories. He did the “rat park” study that found rats deprived of stimulation and social interaction compulsively used drugs, while rats in enriched environments did not.
These understandings are so intuitive, but what if they are wrong?
These narratives make so much sense, and they support other beliefs and agendas many of us hold. Further, it feels like no one is going to harmed by efforts to improve economic, social, and environmental conditions, right?
Well, that’s not quite true. Bill White pointed out that how we define the problem determines who “owns” the problem, and that problem ownership has profound implications for addicts and their loved ones.
Whether we define alcoholism as a sin, a crime, a disease, a social problem, or a product of economic deprivation determines whether this society assigns that problem to the care of the priest, police officer, doctor, addiction counselor, social worker, urban planner, or community activist. The model chosen will determine the fate of untold numbers of alcoholics and addicts and untold numbers of social institutions and professional careers.
The existence of a “treatment industry” and its “ownership” of the problem of addiction should not be taken for granted. Sweeping shifts in values and changes in the alignment of major social institutions might pass ownership of this problem to another group.
White, W. L. (1998). Slaying the Dragon: The History of Addiction Treatment and Recovery in America, page 338
With so many bad actors in treatment right now, there is not a great rush to protect the treatment industry.
To be sure, we’d be better off of a significant portion of the industry disappeared. However, the disappearance of specialty addiction treatment would be tragic for addicts and alcoholics in need of help.
Further, it just so happens that there’s good reason to doubt the “diseases of despair” narrative.
New study casts doubt on “diseases of despair” narrative
A new study looked at county level data and examined the relationship between several economic hardship indicators and deaths by overdose, alcohol-related causes, and suicide.
Mother Jones describes the findings this way:
Economic conditions explained only 8 percent of the change in overdose deaths from all drugs and 7 percent of the change in deaths from opioid painkillers—and even that small effect probably goes away if you control for additional unobservable factors. It explained none of the change in deaths from heroin, fentanyl, and other illegal opioids.
Rising Opioid Deaths: Is the Cause Economic Despair Or Skyrocketing Supply? by Kevin Drum in Mother Jones

They quote the researcher as observing:
Such results probably should not be surprising since drug fatalities increased substantially – including a rapid acceleration of illicit opioid deaths – after the end of the Great Recession (i.e. subsequent to 2009), when economic performance considerably improved.
Rising Opioid Deaths: Is the Cause Economic Despair Or Skyrocketing Supply? by Kevin Drum in Mother Jones
If it’s not economic hardship, what is it?
Vox describes the study’s conclusions this way [emphasis mine]:
. . . the bigger driver of overdose deaths was “the broader drug environment” — meaning the expanded supply of opioid painkillers, heroin, and illicit fentanyl over the past decade and a half, which has made these drugs much more available and, therefore, easier to misuse and overdose on.
Why a better economy won’t stop the opioid epidemic by German Lopez in Vox

Leonid Bershidsky from Bloomberg noted the following:
The absence of an opioid epidemic in Europe indirectly confirms Ruhm’s finding. European nations have experienced the same globalization-related transition as the U.S. In some of them — Greece, Portugal, Ireland, Spain, even France — economic problems were more severe in recent years than in the U.S. Yet no explosion of overdose deaths has occurred.
. . .
There’s also a notable difference in what substances are causing overdose deaths. In the U.S., heroin accounted for 24 percent of last year’s overdose deaths. In Europe in 2018, its share of the death toll was 81 percent. That should say something about how supply affects the outcomes.
Supply, Not Despair, Caused the Opioid Epidemic by Leonid Bershidsky in Bloomberg
Piling on
Then, as if to drive the point home, BMJ posted a study examining the relationship between opioid exposure and misuse. They looked at post-surgical pain treatment,
Each refill and week of opioid prescription is associated with a large increase in opioid misuse among opioid naive patients. The data from this study suggest that duration of the prescription rather than dosage is more strongly associated with ultimate misuse in the early postsurgical period. The analysis quantifies the association of prescribing choices on opioid misuse and identifies levers for possible impact.
Brat G A, Agniel D, Beam A, Yorkgitis B, Bicket M, Homer M et al. Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: retrospective cohort study BMJ 2018; 360 :j5790 doi:10.1136/bmj.j5790
The study “excluded patients with presurgical evidence of opioid or other non-specific forms of misuse in the six months before surgery.” (I would have liked more stringent exclusionary criteria, but it’s still instructive.)
Where does this leave us?
I’ll repeat (a modified version of) what I wrote in a post in response to Johann Hari’s TED talk that emphasized lack of purpose and connection as the cause of addiction and add economic factors to the mix.
- Do economic/social/environmental factors cause addiction? No.
- Are they important? Yes.
- Do they influence the onset and course of addiction? Yes.
- Do they influence the access and responses to treatment? Yes.
- Is addressing those factors important in facilitating recovery for many addicts? Yes.
- Do economic/social/environmental factors cause addiction? No.
Ok, but what about policy?
This leaves us with some uncomfortable (but obvious, to anyone paying attention to this crisis) findings to consider.
Much of the policy discussion over the last several years has been dismissive of supply as a factor in addiction. This poses very serious concerns about that stance.
I’ve never been dismissive of supply as an important consideration, but I am coming to believe that I’ve underestimated its importance.
A lot of that dismissiveness is in response to the drug war and the moral horror of mass incarceration.
The problem demands more of us than we are typically capable of. We need to figure out how to address illicit and licit supply without resorting to mass incarceration/surveillance AND assure treatment of adequate quality, duration, and intensity.
Update
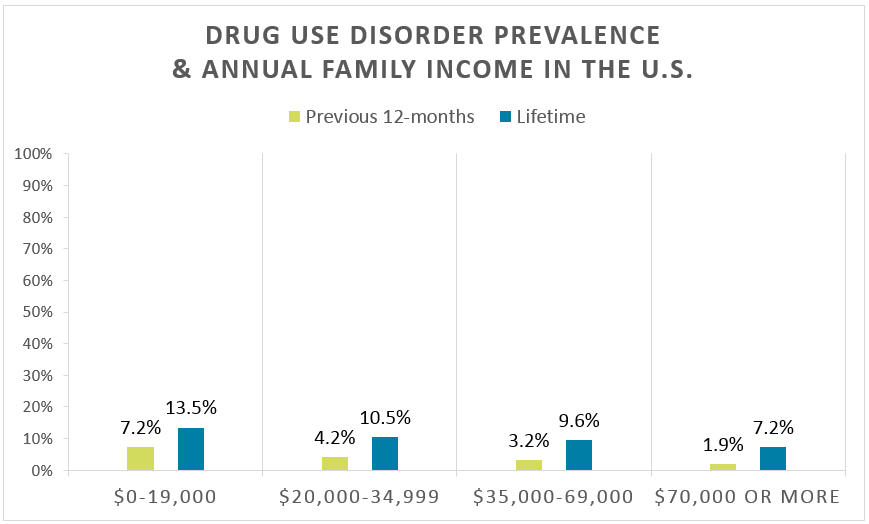
A friend shared this Recovery Research Institute summary of epidemiological data on Substance Use Disorders. (I wish they wouldn’t use addiction and use disorders interchangibley.)
They provide data on SUDs by income, education, geography, age, gender, urban/rural, etc. I don’t see support for the disease of despair narrative in their epidemiological data. Check it out here.

For years, the idea that economic hardship is the primary driver of addiction and overdose has shaped public discourse. But does it truly explain the crisis? As you cite, emerging research suggests that the availability of substances—especially opioids—plays a far greater role than financial struggle alone.
What Are We Missing?
Trauma, not just poverty, fuels substance use. Economic conditions matter, but addiction is more deeply rooted in early childhood adversity, attachment wounds, systemic disenfranchisement, and chronic stress. People don’t just use drugs because they are poor—they use them because their nervous systems are dysregulated, their pain is unresolved, and they lack supportive relationships.
Social disconnection plays a key role. Addiction is often an adaptive response to unmet emotional and relational needs. People use substances to regulate their nervous systems, escape shame, and create a sense of belonging—even if temporary. Addressing addiction requires healing the internal system, not just external conditions.
Where Do We Go from Here?
Instead of focusing solely on despair and economics, we get to implement a trauma-informed, systems-based approach that includes:
✔️ Addressing intergenerational trauma and early adversity as core drivers of addiction.
✔️ Providing relational healing, through community-based models, peer support, and safe spaces that allow for co-regulation.
✔️ Regulating supply with public health in mind, not punitive policies that create more harm.
✔️ Rethinking treatment models—shifting away from outdated paradigms of shame and moral failing toward holistic, compassionate approaches.
The Big Question: Are we willing to move beyond outdated narratives and build solutions that actually heal?
LikeLike
What’s the evidence that trauma is a primary driver of substance use and addiction?
LikeLike
I didn’t say trauma is the only driver, but the evidence overwhelmingly supports it as a major factor. Research in psychology, neuroscience, and sociology consistently links adverse childhood experiences (ACEs), attachment wounds, and chronic stress to higher rates of substance use. Trauma dysregulates the nervous system, leading people to seek substances as a way to self-regulate. This isn’t speculation—it’s well-documented in studies on addiction, complex PTSD, and developmental psychology. Addressing addiction without acknowledging trauma leaves a huge gap in understanding and solutions.
LikeLike
I understood you didn’t call it a sole driver, but you characterized it as a “core” or primary driver and suggested a causal relationship.
I don’t question that trauma, ACEs, and chronic stress influence the risk, onset, course, severity, and response to treatment. That’s different than suggesting a causal relationship.
Of course, a good treatment program should be trauma-informed and, where appropriate, trauma-centered. That’s different than a psychogenic model of addiction that frames addiction as self-medication.
LikeLike
Jason, I appreciate your thoughtful response. I agree—trauma is one of multiple interacting factors, not the sole cause. But I also think we need to acknowledge the extensive research showing how trauma alters brain development, stress responses, and emotional regulation, increasing vulnerability to compulsive behaviors, including substance use.
While addiction is multifaceted, dismissing the role of trauma as merely an ‘influence’ rather than a contributing driver seems to downplay what we know from neuroscience, attachment theory, and somatic psychology. Trauma rewires the nervous system, shaping coping mechanisms—substances included.
That said, I’m not advocating a one-size-fits-all ‘self-medication’ model, but rather an integrated, systems-aware approach that accounts for both structural and individual factors. Trauma doesn’t explain everything, but any framework that ignores it is incomplete.
LikeLike
I wouldn’t call describing a factor as influencing the risk, onset, course, severity, and response to treatment as dismissing that factor. I’m also not sure about the distinction between influencing and being a contributing driver.
I’m also not sure what influential organization or model ignores trauma. I led an organization that became trauma-informed and trauma-responsive through the early 2000s and integration of approaches like EMDR have become common. It’s been a very regular topic in conferences, trade publications, and journals. For example, Seeking Safety is now almost 25 years old, SAMHSA published guidelines for trauma-informed care more than 10 years ago, and ASAM (the most medical of the treatment focused organizations) has several eLearning courses that speak to trauma.
There are a lot of problems that intersect with addiction, including trauma, mental illness, homelessness, criminal justice involvement, poverty, chronic pain, hep C, social isolation, interpersonal violence, etc.
You’ve suggested that there’s a large body of evidence demonstrating that trauma should be centered in treatment and policy responses to addiction. What’s the evidence for that? The post linked to epidemiological data that didn’t, at the population-level, didn’t seem to point toward demographic factors you might point to as associated with trauma and social isolation, particularly if you look at the global level.
LikeLike
Hey Jason, I really appreciate your perspective and your leadership in integrating trauma-informed care early on. You’re absolutely right that addiction intersects with so many systemic issues—trauma, mental health, poverty, and social isolation being just a few.
Where I think we might differ is in how we define what it means to ‘center’ trauma. That doesn’t mean claiming every case of addiction is caused by trauma. But given what we know about how trauma dysregulates the nervous system, disrupts attachment, and increases allostatic load (McEwen, 2000), it’s clear unresolved trauma is a major risk factor for compulsive coping behaviors, including substance use.
A few key points of evidence:
📌 ACE Studies (Felitti et al., 1998; Anda et al., 2006)—Higher ACE scores correlate with increased risk for substance use, depression, and chronic disease.
📌 Van der Kolk (2014)—Explains how trauma alters brain-body regulation, making external substances a way to modulate distress.
📌 Khoury et al. (2010); Boden et al. (2014)—Meta-analyses show PTSD is highly comorbid with addiction and worsens treatment outcomes if not addressed.
📌 SAMHSA Trauma and Justice Initiative (2014)—Lays out how untreated trauma contributes to cycles of addiction, incarceration, and recidivism.
While trauma is widely recognized in the field, policy and funding often don’t reflect that reality. Trauma-focused interventions like EMDR and Seeking Safety exist but aren’t universally embedded in treatment. Many rehab models still focus more on behavior modification than addressing the nervous system dysregulation driving those behaviors. Even harm reduction, while lifesaving, often emphasizes stabilization without deeper healing.
On a global level, factors like drug policy, availability, and cultural attitudes toward distress complicate direct comparisons. But I’d argue that trauma, when left unaddressed, plays a major role in how addiction takes root and persists.
Bottom line: Trauma-informed care can’t just be a box we check in an assessment—it needs to be an active part of treatment. Sustainable recovery isn’t just about stopping a behavior; it’s about healing the nervous system, attachment wounds, and chronic dysregulation.
Would love to hear your take on this!
researchgate.net
(PDF) Social Work and Adverse Childhood Experiences Research
October 21, 2024 — This article provides a selective review of the ACE Study and related social science research to describe how effective social work practice that prevents ACEs
Frontiers
Post-traumatic stress and future substance use outcomes – Frontiers
March 6, 2024 — We conducted an honest causal forest analysis to identify the most important factors that stratify the risk of increased substance use due to …
sites.bu.edu
The Adverse Childhood Experience (ACE) Study | Danielle Rousseau
December 11, 2023 — The ACE study (van der Kolk, 2014) revealed that childhood and adolescence are particularly vulnerable times for traumatic experiences.
delanceyplace.com
the gravest health crises of our time — 2/6/19 – Delancey Place
February 5, 2019 — “Felitti and Anda spent more than a year developing ten new questions covering carefully defined categories of adverse childhood experiences, …
healthandjusticejournal.biomedcentral.com
Action steps using ACEs and trauma-informed care: a resilience model
April 27, 2017 — This paper 1) discusses two important contributions that are shaping work with vulnerable and under-resourced populations.
acestoohigh.com
The Adverse Childhood Experiences Study — the largest, most …
October 2, 2012 — To explain this, Anda and Felitti developed a scoring system for ACEs. Each type of adverse childhood experience counted as one point. If a …
PubMed
Relationship of childhood abuse and household dysfunction to …
We found a strong graded relationship between the breadth of exposure to abuse or household dysfunction during childhood and multiple risk factors.
PubMed
Substance use, childhood traumatic experience, and Posttraumatic …
The present study further examines this relationship between childhood trauma, substance use, and PTSD in a sample of urban primary care patients.
PubMed
Psychological interventions for post-traumatic stress disorder and …
We concluded that there is evidence that individual trauma-focused psychological intervention delivered alongside SUD intervention can reduce PTSD severity, and …
PubMed Central
The enduring effects of abuse and related adverse experiences in …
The ACE Study included 17,337 adult HMO members and assessed 8 adverse childhood experiences (ACEs) including abuse, witnessing domestic violence, and serious …
library.samhsa.gov
[PDF] Trauma-Informed Care in Behavioral Health Services Part 3
Providing a comprehensive literature review on trauma, traumatic stress, trauma-informed care. (TIC), and trauma-related interventions is a daunting task …
library.samhsa.gov
[PDF] Practical Guide for Implementing a Trauma-Informed Approach
SAMHSA is committed to improving prevention, treatment, and recovery support services for individuals with mental illnesses and substance use disorders.
library.samhsa.gov
[PDF] SAMHSA TIP 33 Treatment for Stimulant Use Disorders
The results are tremendous advances in understanding stimulant use disorders, the basic functioning of the brain, and substance use disorders (SUDs) in general.
istss.org
Psychotherapy Interventions for Co-occurring PTSD and Substance …
Important advances in the psychosocial treatment of posttraumatic stress disorder (PTSD) and substance use disorders (SUD) have occurred over the past two …
researchgate.net
Adverse childhood experiences: Towards a clear conceptual meaning
Adverse childhood experiences have been associated with negative physical and psychological health outcomes, but this phenomenon lacks the clear, consistent …
cpeip.fsu.edu
[PDF] ACE Study Publications Published 1. Felitti VJ, Anda RF …
Several books focused on the material of the ACE Study have recently been published, most notably van der Kolk’s “The Body Keeps the Score”, Nakazawa’s “ …
uclaisap.org
[PDF] SAMHSA TIP 33 Treatment for Stimulant Use Disorders
The Treatment Improvement Protocol (TIP) series contributes to SAMHSA’s mission by providing science- based, best-practice guidance to the behavioral health …
Amazon
The Body Keeps the Score: Brain, Mind, and Body in the Healing of …
Van der Kolk offers a wealth of exercises and strategies that readers can incorporate into their daily lives to regulate their nervous system.
LikeLike
Thanks. I’m familiar with ACEs, Van der Kolk, and I referred to SAMHSA’s work in my last comment.
Did you review Khoury and Boden? Khoury’s paper has a very complicated, multi-problem group of subjects. They do have elevated rates of AOD problems, but the number of problems and complexity of the subjects make it hard to generalize.
Boden selected for subjects who were veterans with current alcohol or drug use disorder and meeting full or partial criteria for PTSD. It looked at coping patterns and response to treatment. It actually found similar improvements with Seeking Safety and treatment as usual. The trauma focused model performed no better than treatment as usual in that study.
Other papers you cite don’t report any original findings or only tangentially mention addiction or substance use, Larkin for example.
I don’t see how this demonstrates trauma is a “core driver” of addiction or that addiction is “deeply rooted” in trauma. Or, that it’s incorrect or inadequate to say “trauma, ACEs, and chronic stress influence the risk, onset, course, severity, and response to treatment.”
It’s important. It influences addiction and treatment. So do mental illness, homelessness, criminal justice involvement, poverty, chronic pain, social isolation, interpersonal violence, etc.
Your references to SAMHSA demonstrate the attention trauma gets. Najavits reported that in 2009, 2/3 of 13,223 substance abuse treatment facilities reported using “trauma counseling” sometimes or always or often. Who knows what they were referring to, but that was 16 years ago!
LikeLike
Jason, I appreciate the depth of your response and your engagement with the evidence. You raise valid points, and I want to be clear—I’m not arguing that trauma is the sole driver of addiction, nor that every person with a substance use disorder has trauma at its core. But I do maintain that unresolved trauma is a key driver for a significant subset of people struggling with addiction.
You’re absolutely right to scrutinize studies like Khoury and Boden. They do have methodological limitations, but they also reflect a larger trend—high rates of comorbidity between PTSD and substance use disorders (SUDs), as well as the influence of trauma on self-regulation and coping mechanisms. The mixed outcomes in trauma-focused treatments, as you noted, highlight an important issue: while trauma matters, simply adding trauma-informed elements to existing models isn’t necessarily transformative without deeper systemic change.
What I find compelling isn’t just the treatment outcomes but the biological and psychological mechanisms linking trauma to compulsive behaviors, including addiction:
📌 Dysregulated stress response (McEwen, 2000)
📌 Altered reward processing & impulse control (Koob & Volkow, 2010)
📌 Attachment disruption and self-regulation difficulties (Schore, 2001; Porges, 2011)
As for the widespread adoption of trauma-informed care in treatment settings, I agree—there’s been progress. But the reality is that “trauma-informed” is often superficial, with many programs still operating from behavioral modification frameworks rather than deeply integrative, nervous system-aware models. Trauma isn’t just a factor—it can be the organizing principle behind why some people develop entrenched substance use patterns while others do not.
So, my core argument is this:
1️⃣ Trauma is a major but often inadequately addressed driver of addiction (though not the only one).
2️⃣ Addiction treatment must go beyond symptom suppression—we need deeper interventions that engage the nervous system, attachment wounds, and identity reconstruction.
3️⃣ Addressing trauma isn’t just about adding a module to treatment—it’s about fundamentally shifting how we understand and engage with addiction.
Would love to hear your thoughts on how we close the gap between trauma-awareness and true trauma-responsive care in addiction treatment.
LikeLike
Thank you very much for an interesting, well-researched, and relevant post. No, for a long time, it has been comme il faut to overlook the accessibility/supply factor.
Regarding the discussion on trauma, based on what is written here, it is impossible to determine what the author means by “trauma.” Is it an unpleasant/life-threatening experience, or is it the potential consequences (such as PTSD, which only a minority develop) that are being considered in the descriptions and references to the literature?
It is difficult to measure—for example, childhood experiences. Retrospective studies, such as ACE, rely on notoriously unreliable memory, particularly among individuals currently facing significant health problems. These individuals may have a need to find an explanation that absolves them of personal responsibility for their present situation.
Liese
LikeLike
Thank you very much for an interesting, well-researched, and relevant post. No, for a long time, it has been comme il faut to overlook the accessibility/supply factor.
Regarding the discussion on trauma, based on what is written here, it is impossible to determine what the author means by “trauma.” Is it an unpleasant/life-threatening experience, or is it the potential consequences (such as PTSD, which only a minority develop) that are being considered in the descriptions and references to the literature?
It is difficult to measure—for example, childhood experiences. Retrospective studies, such as ACE, rely on notoriously unreliable memory, particularly among individuals currently facing significant health problems. These individuals may have a need to find an explanation that absolves them of personal responsibility for their present situation.
Liese
LikeLike