
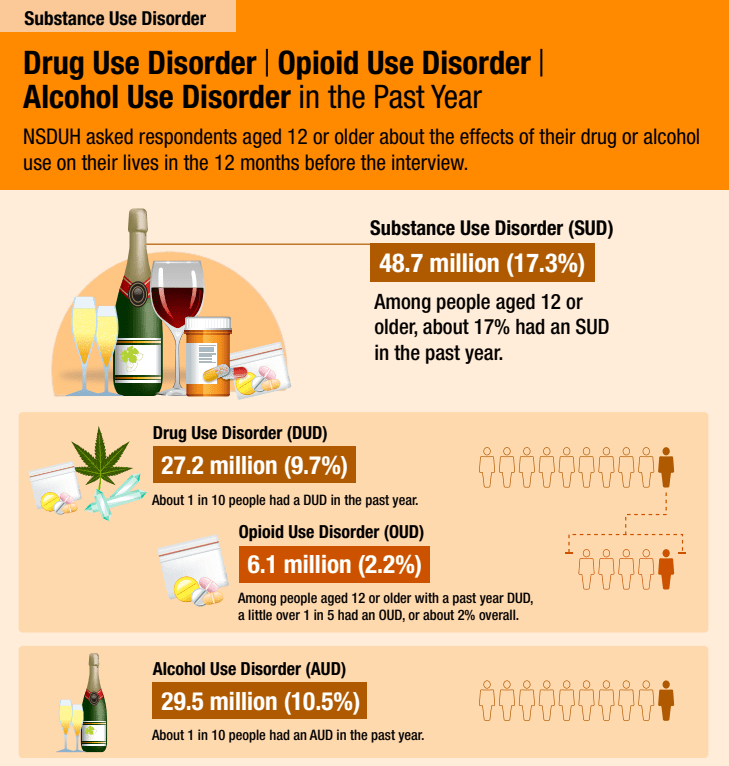
The 2022 National Survey on Drug Use and Health was recently released and it reports, using DSM-5 criteria, that 17.3% of Americans 12 or older (48.7 million people) had a substance use disorder (SUD) in the past year.
For context, the 2020 National Survey on Drug Use and Health, the first year using DSM-5 criteria, reported that 14.5% of Americans 12 or older had a substance use disorder (SUD) in the past year.
And, according to the 2012 National Survey on Drug Use and Health, using DSM-IV criteria, 8.5% of Americans 12 or older met criteria for past-year Alcohol or Drug Dependence or Abuse.
At what point do we recognize that the term substance use disorder doesn’t tell us much? It’s too inclusive to mean much of anything.
How high will it go? If more than one in six Americans 12 or older have a past year SUD, what’s the lifetime prevalence?
As a category, SUD is about as helpful as pulmonary disease. It tells you something about the likely symptoms, but it could be acute, it could be chronic, it could be mild, it could be severe, it could be a minor inconvenience, or it could be disabling and something that shapes the person’s identity.
It tells us nothing about the nature of the problem, the cause, the course, the severity, whether it requires treatment, the kind of treatment indicated, what problem resolution (recovery) looks like, or the implications for the patient, their loved ones, and the community.
Of course, this isn’t news and it’s not without consequence.
But, there is a way to differentiate chronic and severe problems from other types of SUDs.
One more thought: Maybe SUD is useful at the population level. If that’s true, what are the consequences of a diagnostic category that is much more useful at a population level and not particularly useful for treatment? What pressures does that create for treatment systems? What blindspots does it create for systems of care?
